

BREAKING: Peer-Reviewed Paper Finds mRNA “Vaccines” Convey Silent Heart Damage — Presents Approach to Diagnosis and Management
We present the first-ever paper to map the symptoms, diagnosis, and treatment of COVID-19 vaccine-induced subclinical myopericarditis — the silent condition driving “unexplained” sudden deaths.

For years, COVID-19–vaccinated people have collapsed or died suddenly with “no explanation” — athletes on the field, young adults in their sleep, and otherwise healthy individuals with no prior heart history. Our new peer-reviewed paper titled, COVID-19 Vaccine-Induced Subclinical Myopericarditis: Pathophysiology, Diagnosis, and Clinical Management, published in the European Society of Medicine’s Medical Research Archives, finally connects the dots — and provides real solutions.
A silent epidemic of subclinical myopericarditis and heart injury is occurring beneath the surface — often without symptoms, without warning, and in some cases, with sudden cardiac arrest as the first sign of disease.
This is the first peer-reviewed paper to formally define, characterize, and clinically map COVID-19 vaccine-induced subclinical myopericarditis. We establish the first unified diagnostic and risk-stratification framework for identifying subclinical cases — and present the first structured management and detoxification protocol aimed at reducing ongoing Spike-mediated cardiac injury.
What is COVID-19 vaccine-induced subclinical myopericarditis?
Subclinical myopericarditis is heart inflammation caused by COVID-19 mRNA vaccination that occurs without the classic warning signs seen in overt myocarditis. Instead of dramatic chest pain or hospitalization, the injury unfolds silently — detectable only through biomarkers, ECG changes, imaging, or antibody/spike measurements.
What Makes It “Subclinical”?
Unlike traditional myocarditis, which presents with obvious symptoms, subclinical vaccine-induced myopericarditis:
Produces measurable myocardial injury (troponin, BNP, galectin-3, D-dimer)
Often shows ECG abnormalities (ST/T-wave changes, arrhythmias)
Can involve pericardial inflammation (thickening or small effusions)
May show patchy fibrosis or edema on cardiac MRI
Is usually missed unless specifically screened for
Because affected individuals appear outwardly healthy, this condition is vastly underdiagnosed.
Broad Clinical Manifestations
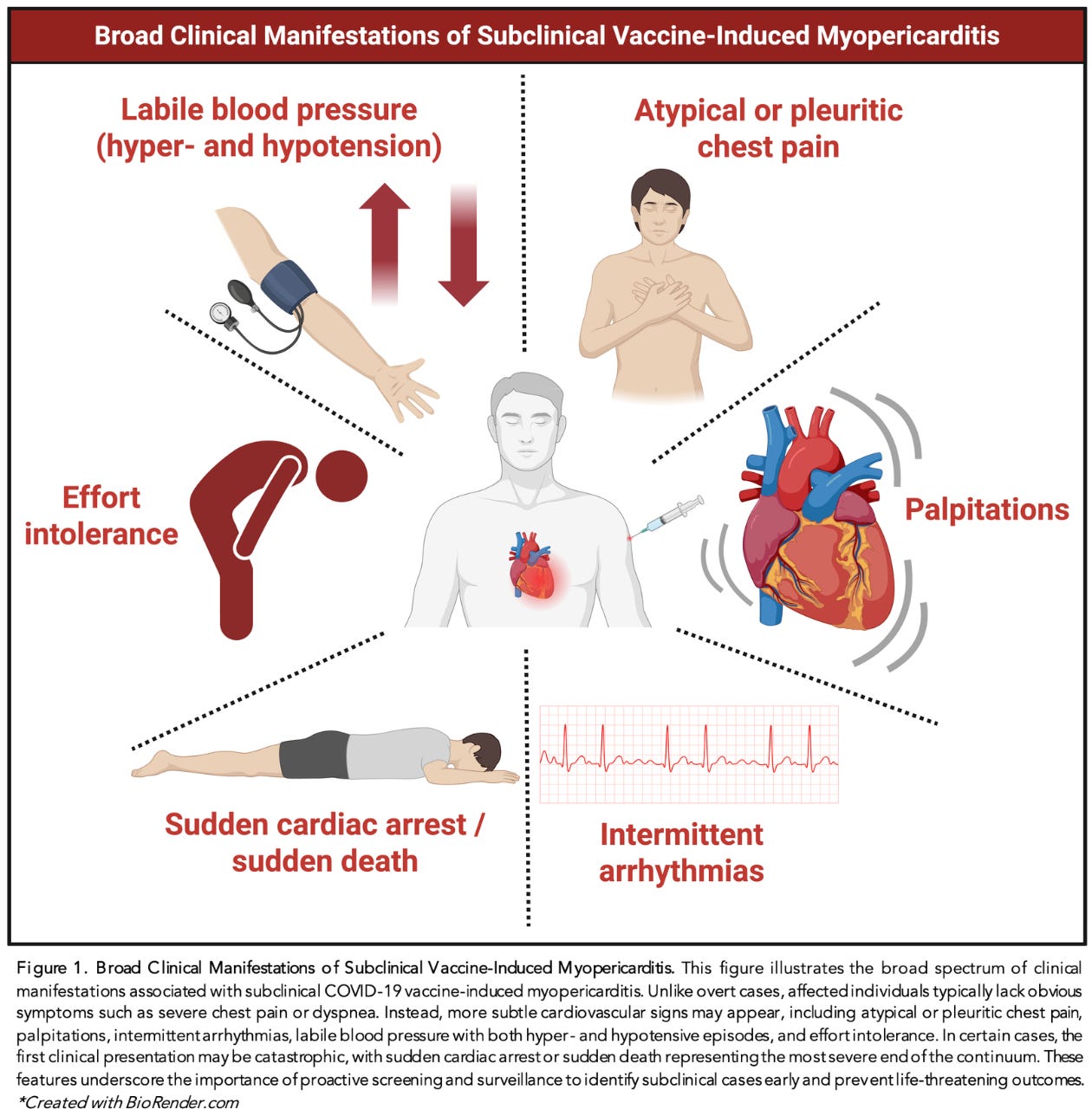
The spectrum of subclinical myopericarditis is broader — and more dangerous — than the public has been told. Based on the evidence synthesized in the paper, individuals may experience:
Subtle or Intermittent Symptoms
Atypical or pleuritic chest pain
Palpitations or “fluttering” sensations
Intermittent arrhythmias
Effort intolerance
Labile blood pressure (episodes of hyper- OR hypotension)
Heart-rate instability, including POTS-like patterns
Laboratory & Imaging Clues
Mild–moderate troponin elevation
Elevated BNP, galectin-3, D-dimer
ECG: ST-segment changes, ectopy, irregular rhythms
MRI: late gadolinium enhancement (LGE), edema, or subtle inflammatory patterns
Biologic Evidence of Injury
Persistent circulating Spike protein
Detection of vaccine mRNA in heart tissue
Extremely elevated quantitative Spike antibodies, indicating high cumulative exposure
In some individuals, the initial manifestation may be catastrophic: Sudden cardiac arrest without any prior symptoms.
Autopsy studies show microscopic inflammatory scars too small for MRI to detect, yet fully capable of triggering lethal arrhythmias.
1–3% of COVID-19 Vaccine Recipients May Have Sustained Heart Damage
The emerging evidence suggests that silent heart damage after mRNA vaccination is far more common than health authorities acknowledged. Based on prospective studies and symptom surveillance, a meaningful percentage of recipients — especially younger individuals — may have experienced measurable myocardial injury without ever knowing it. As we outline in the paper:
“The incidence of subclinical myopericarditis is challenging to estimate, as it requires sensitive screening and is not associated with symptoms that would prompt clinical evaluation. Chiu et al found among 763 students a rate of 17.1% had at least one cardiac symptom after the second vaccine dose, mostly chest pain and palpitations. Three prospective cohort studies have evaluated the incidence of subclinical myopericarditis after injection of synthetic mRNA. Mansanguan et al. reported an incidence rate of 2.3%, Buergin et al. reported an incidence rate of 2.8%, and a Pfizer-sponsored study yielded an estimated incidence rate of 1.0%, though that study omitted daily cardiac troponin measurements. It is reasonable to surmise that approximately 1–3% of COVID-19 mRNA vaccine recipients suffer some degree of myocardial injury per dose, thereby representing a profound concern for the short- and long-term health of younger vaccinees.”
When applied across millions of doses, a 1–3% injury rate translates into millions of individuals with unrecognized cardiac damage — underscoring the urgent need to take subclinical myopericarditis seriously and to implement proper diagnostic and treatment pathways.
Management
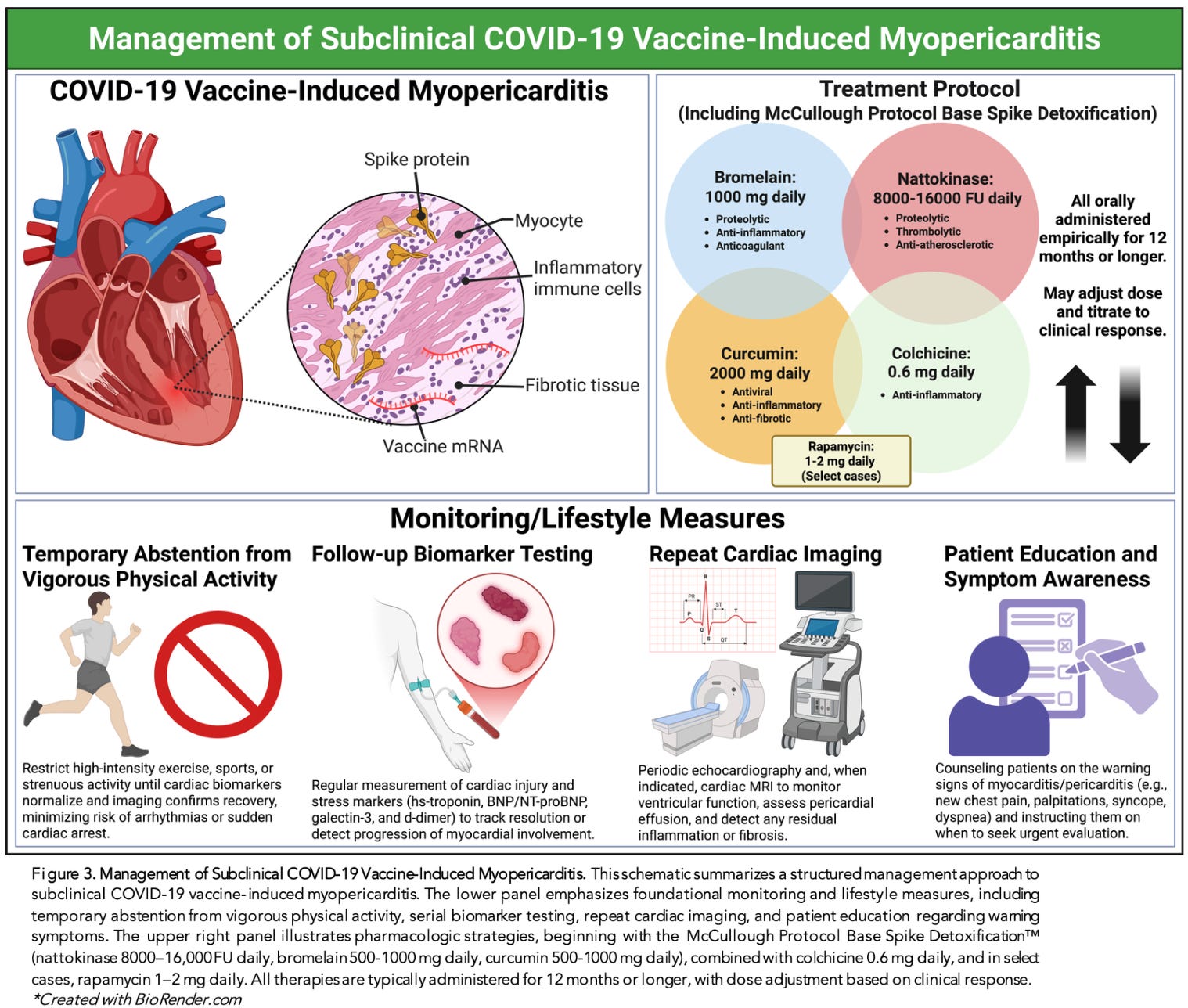
Our paper outlines the first structured clinical management pathway for subclinical myopericarditis following COVID-19 mRNA vaccination. This framework — summarized in Figure 3 of the publication — integrates lifestyle precautions, biomarker surveillance, imaging follow-up, and targeted pharmacologic intervention.
1. Foundational Monitoring & Lifestyle Measures
The first priority is to avoid exacerbating myocardial inflammation, prevent arrhythmic triggers, and track the trajectory of recovery. Recommended foundational steps include:
Temporary abstention from vigorous physical activity
Strenuous exercise increases catecholamines and can precipitate arrhythmias or sudden cardiac arrest in inflamed myocardium.Serial biomarker testing
Repeated troponin, BNP, galectin-3, and D-dimer measurements help determine whether myocardial injury is resolving or persisting.Repeat cardiac imaging
Echocardiograms and, when indicated, cardiac MRI are used to monitor ventricular function, pericardial effusion, and fibrosis.Patient education on warning symptoms
Individuals must be taught to watch for palpitations, chest discomfort, blackouts, blood-pressure instability, or decreased exercise tolerance — all signs of potential deterioration.
These conservative measures form the base layer of long-term care.
2. Spike Detoxification & Pharmacologic Therapy
The second layer of management focuses on clearing persistent Spike protein, reducing inflammation, and preventing progression to chronic fibrosis or arrhythmic risk. The paper details a structured, multi-agent approach:
McCullough Protocol Base Spike Detoxification
A targeted 3-part regimen designed to degrade circulating Spike protein and reduce inflammatory load:
Nattokinase: 8,000–16,000 FU daily
Bromelain: 500–1000 mg daily
Curcumin: 500–1000 mg daily
These agents work synergistically to enhance proteolysis, modulate endothelial inflammation, and support microvascular recovery.
Colchicine (0.6 mg daily)
Evidence supports colchicine in reducing pericardial and myocardial inflammation. It is recommended for most moderate or persistent subclinical cases.
Rapamycin (1–2 mg daily; select refractory cases)
For prolonged or relapsing inflammation, rapamycin offers mTOR inhibition that can:
reduce immune hyperactivation,
limit fibrotic remodeling, and
restore cellular homeostasis.
Its use is generally reserved for severe cases with documented ongoing myocardial involvement.
3. Duration of Therapy
All components of management — lifestyle, monitoring, detoxification, and medications — are typically continued for 12 months or longer, with dosage and duration tailored to:
biomarker normalization,
imaging resolution,
symptom trajectory, and
overall clinical response.
This recognizes the chronic nature of Spike persistence and the long healing times required for inflamed myocardium.
Conclusion
COVID-19 vaccine-induced subclinical myopericarditis represents a silent, widespread, and devastating form of cardiac injury. Countless indidvuals around the world are now living with undiagnosed heart inflammation — without obvious warning signs.
This paper finally gives clinicians the diagnostic tools, risk framework, and management strategies needed to identify and treat this condition. It closes a gap that should never have existed — a gap created by regulatory agencies that refused to investigate, refused to monitor, and refused to acknowledge the scale of vaccine-induced injury.
What the CDC should have done, the McCullough Foundation is doing.
For four years, regulators ignored the vaccine-injured and failed to develop any clinical guidance. The McCullough Foundation stepped in to fill the vacuum — conducting the research, publishing the papers, and building the pathways they would not. We will continue finding real solutions for the millions of vaccine-injured worldwide.
But this work depends on independent support. If you believe in this mission and want to help accelerate urgent research, clinical protocols, and public education, please consider donating to the McCullough Foundation: https://mcculloughfnd.org/products/donate-1
The institutions that caused this crisis have abandoned the injured. We will not.

Epidemiologist and Foundation Administrator, McCullough Foundation
Support our mission: mcculloughfnd.org
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.
Its amazing that many doctors today can see all the carnage going on...with masses of people being injured and dying..and they keep on pushing vaccines. Didn't they learn that POISON kills and the matter in all VACCINES is toxic to the human body? What's going on is plain MURDER!
I must not have any of this since I am over 75 and was shoveling some wet heavy snow yesterday with no trouble. Of course, I have not had any vaccinations in over 50 years and I sometimes think about mRNA shedding. If it is real and all. The doctors have no clue.
However, nowadays no research papers can be trusted even if they go against the medical mafia. Peer reviewed is code for I'll scratch your back if you scratch mine.