

Hantavirus Outbreak on MV Hondius Cruise Ship
Latest reporting on the unhappy voyage.

Passengers and crew are still confined on board the MV Hondius, following a deadly outbreak of hantavirus over a month ago. The vessel—named after Jodocus Hondius (1563–1612) a renowned Flemish-Dutch engraver, cartographer, and publisher—departed Ushuaia, Argentina, on April 1, 2026, carrying approximately 147 passengers and crew on a polar itinerary through the South Atlantic, including stops in Antarctica, South Georgia, and remote islands like Tristan da Cunha and Saint Helena.

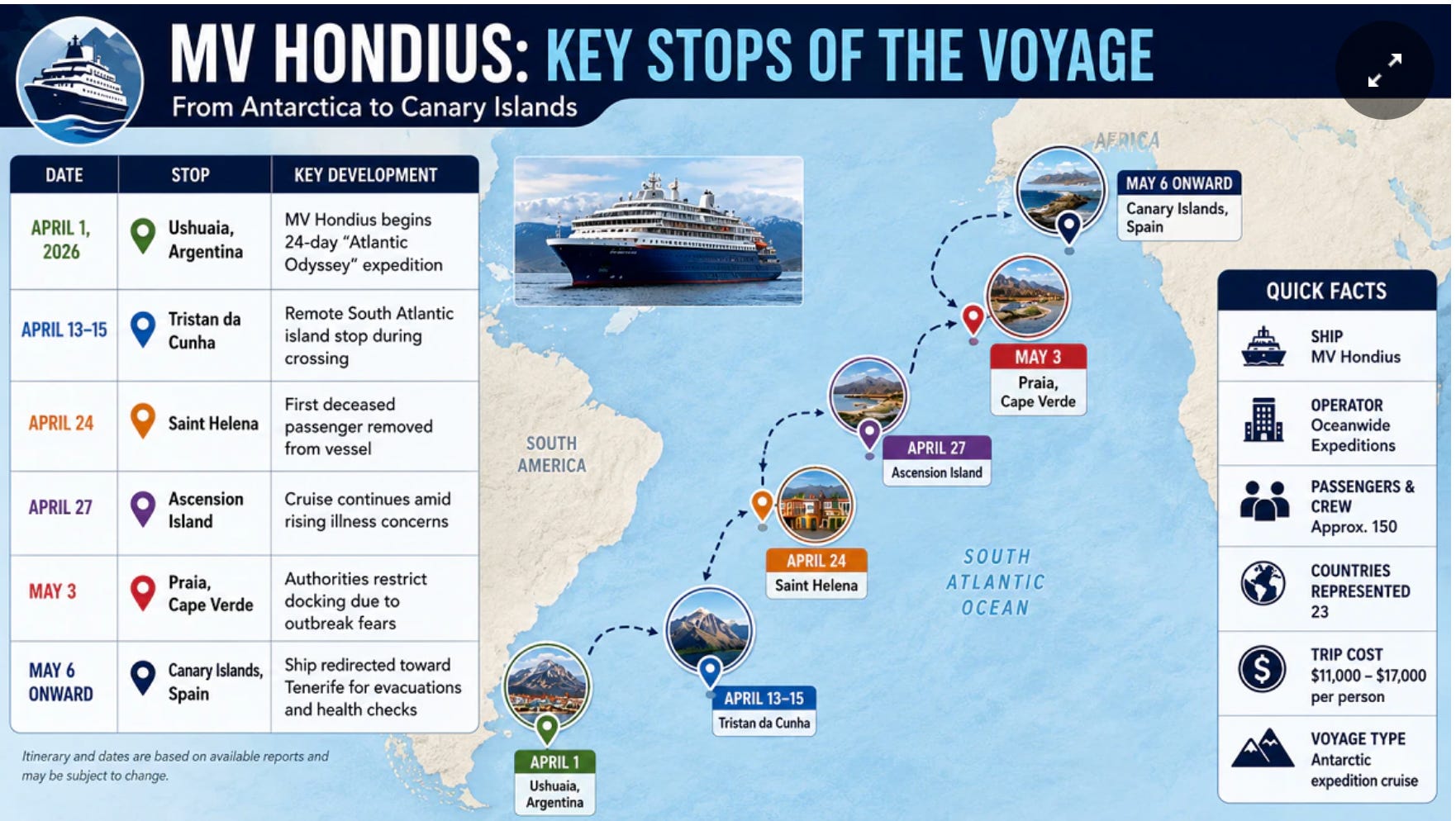
Their infernal odyssey has unfolded on the following timeline.
April 1, 2026: The MV Hondius departs Ushuaia, Argentina, for a polar voyage.
April 6, 2026: First symptoms are reported by passengers.
April 11, 2026: A 70-year-old Dutch passenger dies. His death is initially attributed to natural causes. Doctors on board initially believe the illness is not infectious, so dozens of passengers are permitted to disembark as planned at St. Helena on April 24 without screening or contact tracing. After these passengers travel globally, health authorities confirm the presence of hantavirus on board the ship.
April 25, 2026: The 69-year-old Dutch wife of the deceased man boards a KLM flight from Johannesburg to Amsterdam but is then escorted off the plane after crew members assessed her deteriorating medical condition. She subsequently dies in Johannesburg.
Late April – Early May: Ship is denied entry at Cape Verde, remains at anchor while authorities organize emergency medical evacuations.
May 6, 2026: Three individuals—including the ship’s doctor—are medically evacuated and flown to the Netherlands for treatment.
May 6, 2026: A flight attendant on the KLM flight from Johannesburg to Amsterdam who encountered the Dutch wife of the initial fatal case is admitted to hospital in Amsterdam. She is the first suspected infection outside the passengers and crew of the ship.
May 7, 2026: The MV Hondius has departed Cape Verde and is currently en route to Tenerife (Canary Islands) where it is expected to arrive around May 10.
Passengers are to undergo a medical assessment onboard. Those with no symptoms are to be repatriated to their home countries, starting around May 11. Spanish nationals are to be quarantined in a military hospital in Madrid. Evacuations would use protective equipment, with no direct contact with local Canary Islands residents. The ship will likely remain at anchor or with minimal port time.
Spain’s central government (via Health Minister Mónica García) approved this despite local opposition from Canary Islands officials, who are characterizing it as “reckless.” Authorities claim the disembarkation of the remaining passengers poses little risk to the public, as no one currently onboard is currently presenting symptoms.
What Are Hantaviruses
Hantaviruses are a group of viruses of the family Hantaviridae, order Bunyavirales, with the primary human-pathogenic species classified under the genus Orthohantavirus. The rodent-borne viruses are known to cause severe diseases, including Hantavirus Pulmonary Syndrome (HPS) in the Americas and Hemorrhagic Fever with Renal Syndrome (HFRS) in Eurasia.
Symptoms of hantavirus infection can include fever, extreme fatigue, muscle aches, stomach pain, nausea, vomiting, and and shortness of breath. In some cases, people develop severe breathing difficulties requiring hospitalization. Symptoms usually appear between 2 to 4 weeks after being exposed to the virus, but there are reports of symptoms occurring up to 40 days after exposure.
The first hantavirus (specifically the Hantaan virus) was isolated by Ho-Wang Lee and his colleagues in South Korea in 1978 from the striped field mouse (Apodemus agrarius) near the Hantan River, thereby identifying the causative agent of Korean hemorrhagic fever.
Laboratory testing of samples from the ship confirmed the strain as Andes virus (Andes orthohantavirus), a New World hantavirus endemic to southern South America (primarily Argentina and Chile) and carried by the long-tailed pygmy rice rat (Oligoryzomys longicaudatus).

This matches the geographic origin and explains the clinical presentation of hantavirus pulmonary syndrome (HPS), characterized by fever, respiratory distress, and high fatality.
Andes virus is distinguished for its rare capacity for limited human-to-human transmission, documented in small clusters in Argentina and Chile. Notable precedents include the 1996 El Bolsón outbreak (16 linked cases) and the 2018–2019 Epuyén event in Patagonia (34 confirmed infections, 11 deaths), where transmission occurred via close household or intimate contact.
Origin of the Outbreak
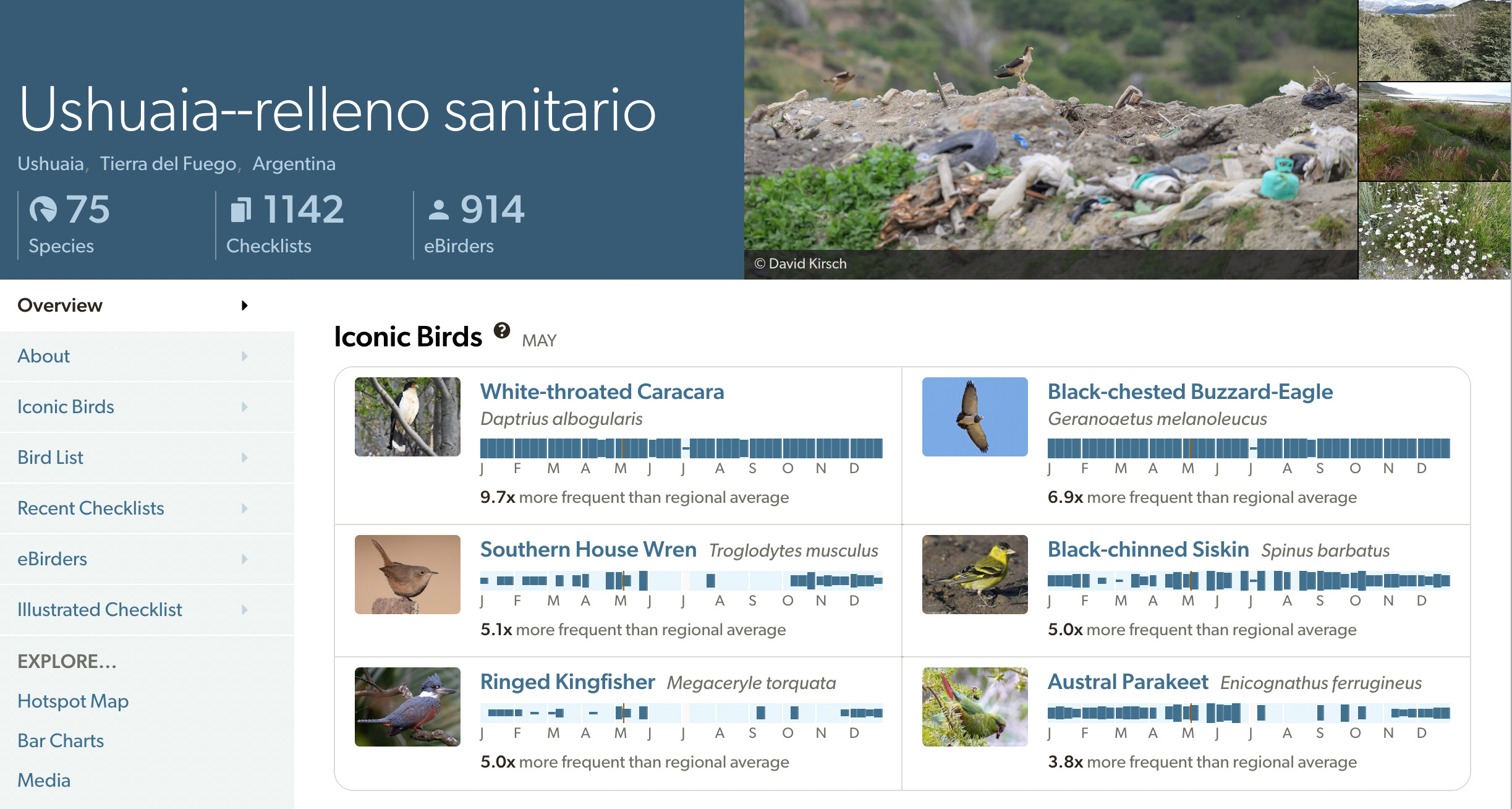
Investigators claim they have traced the likely index cases to rodent exposure prior to boarding. The Dutch couple—the first fatalities—is said to have contracted the virus during a pre-cruise bird-watching excursion in Ushuaia, Tierra del Fuego that included a visit to a local landfill, where they may have inhaled aerosolized particles from infected rodent urine, feces, or saliva. If this is indeed the case, they apparently presented symptoms in an unusually short period after their exposure.
Research reveals that the Ushuaia relleno sanitario landfill is indeed a birdwatching hotspot. The White-throated Caracara (Phalcoboenus albogularis or Daptrius albogularis) is the primary “lifer” target—that is, the first time a bird will be viewed by a dedicated birdwatcher. This species of Caracara is typically only seen only at the Ushuaia dump (or similar sites) in southern South America, where it scavenges and associates with other caracaras
Argentina’s health ministry claims it is trapping rodents in the area to confirm this hypothesis. The ship’s departure from southern Argentina aligns with the endemic range of the identified pathogen.
So far, I have seen no reports of a rodent infestation being discovered aboard the vessel, but I can’t help but wonder about this. Though modern cruise ships employ strict procedures for preventing rodents from boarding, it can still happen. Rodents can hide in wooden pallets or cardboard boxes during the loading of food and supplies. Rats are capable of scurrying up docking lines, though most ships use rat guards—conical or circular shields—on these lines to block them from reaching the hull. Rodents have also been known to hitch a ride inside suitcases or shopping bags from port cities.
Comparison to Historical Outbreaks
Hantavirus infections are rare globally and almost always zoonotic. Major historical events include the 1993 Four Corners outbreak in the southwestern United States (Sin Nombre virus, ~50 initial cases, ~50% fatality) and sporadic cases of hemorrhagic fever with renal syndrome (HFRS) in Asia and Europe.
In the Americas, Andes virus has caused hundreds of HPS cases since its identification in 1995, with case fatality rates of 20–50%.
The MV Hondius outbreak is unprecedented as the first recorded hantavirus cluster on a cruise ship and one of the largest suspected human-to-human events outside South America. It is consistent with the confined, prolonged contact of prior Andes clusters (e.g., family or healthcare settings) but peculiar in its occurrence in a travel setting with passengers from multiple continents. Unlike typical cruise-ship outbreaks (e.g., norovirus, which spreads efficiently via fecal-oral routes), this event highlights the virus’s dependence on specific exposure conditions rather than broad airborne contagion.
Virulence, Transmissibility, and Variant Status
According to various media reports, the cases onboard the ship do not indicate exceptional virulence or transmissibility compared to other hantavirus clusters. Fatality (~40% in confirmed cases) and clinical severity are consistent with known Andes virus HPS outcomes. Human-to-human spread, while suspected as a factor in secondary onboard infections, remains limited and is said to require close, prolonged contact—consistent with all prior Andes documentation.
The WHO has repeatedly stated that the risk to the general public is low; the virus is not easily transmitted casually, and no community spread has been detected beyond ship contacts. Global monitoring of disembarked passengers (including Americans, Europeans, and others) has identified no further outbreaks.
The WHO claims there is no evidence that the virus is a new mutant variant. Genetic sequencing shows the strain is virtually identical (>99% match) to established Andes virus lineages circulating in Argentina. WHO officials claim they have ruled out mutations enhancing transmissibility or virulence at this stage. Ongoing genomic analysis continues, but current data are said to indicate a standard, endemic strain introduced via the pre-boarding exposure.
It’s a hell of thing to contemplate being stuck aboard a ship for weeks on end, unwelcome in any port. The episode recalls the origin of the word quarantine—from the Italian phrase quaranta giorni, meaning "forty days.”
The practice traces back to the 14th century, during the time of the Black Death, when it was used to describe the mandatory 40-day isolation period imposed on ships and travelers to prevent the spread of the plague. In the European context, the practice was instituted by the Republic of Venice, which called it it quarantena. Ships were directed to dedicated island stations in the Venetian Lagoon to primarily the Lazzaretto Nuovo for suspected cases and cargo, and the Lazzaretto Vecchio for the actively sick.
It seems to me that an open-air refugee camp with widely spaced tents for shelter and sleeping would be preferable to confining the passengers to the ship’s rooms for weeks on end. In tents widely separated from others, each passenger could get plenty of sunlight and breathe fresh air far enough apart from other passengers to avoid transmission. Each could then be released after showing no symptoms for a prescribed period and obtaining negative antibody or PCR tests.
John - I want you to examine the possibilities that viruses do not exist. This is known knowledge since polio — but not mainstream because mainstream needs fear and pandemic.
I’ve written three pieces on this, here’s there first one: https://unorthodoxy.substack.com/p/why-disease-causing-viruses-are-pseudoscience
Thanks for clearly reporting the official story. I encourage you all to be highly skeptical of these Media fueled outbreaks. I have been following them for 30 years and every time you look deeply you find the story falls apart.
In the past 20 years the problem has become much worse because of reliance on highly unreliable PCR tests.
. A good place to start is sexual transmission of HIV. The research study cited below was published in the American Journal of epidemiology in 1997. It remains the highest quality study ever done on the subject. Although the abstract claims that it takes 1000 sexual contacts to transmit HIV (“ Per contact infectivity 0.0009“), which is astounding by itself, when you read the text of the article you find that despite following 175 couples over the course of their study, zero of the HIV negative partners changed to HIV positive. This despite very inconsistent use of “safe sex“ among the couples.
I will add that just because someone turns from HIV negative HIV positive does not mean that they “caught it” from someone. When a person’s system is activated by allergy, autoimmune conditions, exaggerated reactions to vaccines or other stimuli, people are very likely to turn from HIV negative to HIV positive, although not always permanently.
There is a very similar study on IV drug use. People using exclusively clean needles from a needle exchange program had a dramatically higher chance of testing HIV positive than people who used shared needles. This was also published in the American journal of epidemiology in 1997. However these studies appeared after 13 years of the same narrative that had created and bolstered many careers, belief systems, research grants and salaries, so people just ignored these landmark studies.
Nancy S. Padian, Stephen C. Shiboski, Sarah O. Glass, Eric Vittinghoff, Heterosexual Transmission of Human Immunodeficiency Virus (HIV) in Northern California: Results from a Ten-year Study, American Journal of Epidemiology, Volume 146, Issue 4, 15 August 1997, Pages 350–357, https://doi.org/10.1093/oxfordjournals.aje.a009276