

Professor Didier Raoult & Hydroxychloroquine
Nicholas Hulscher's exposition of HCQ's anti-viral property reminded me of the seminal work of the great French microbiologist and master of repurposed drug therapies.

I just watched the following interview with McCullough Foundation epidemiologist Nicholas Hulscher.
Nic’s exposition reminded me of the seminal work of Professor Didier Raoult, who has long struck me as one of the most original, creative, and penetrating minds in all of microbiological research. Professor Raoult conducted the seminal study of hydroxychloroquine as a potent inhibitor of SARS-CoV-2 — an extremely valuable service to mankind for which he was relentlessly persecuted by the French public health authorities. These same authorities had — in one of the most curious and intriguing elements of the official organized criminal pandemic response — inexplicably removed HCQ’s over-the-counter availability in France shortly before the pandemic began.
If you are not already familiar with the fascinating life and work of Professor Raoult, you will find the following chapter from my book (with Peter A. McCullough, MD) informative and entertaining.
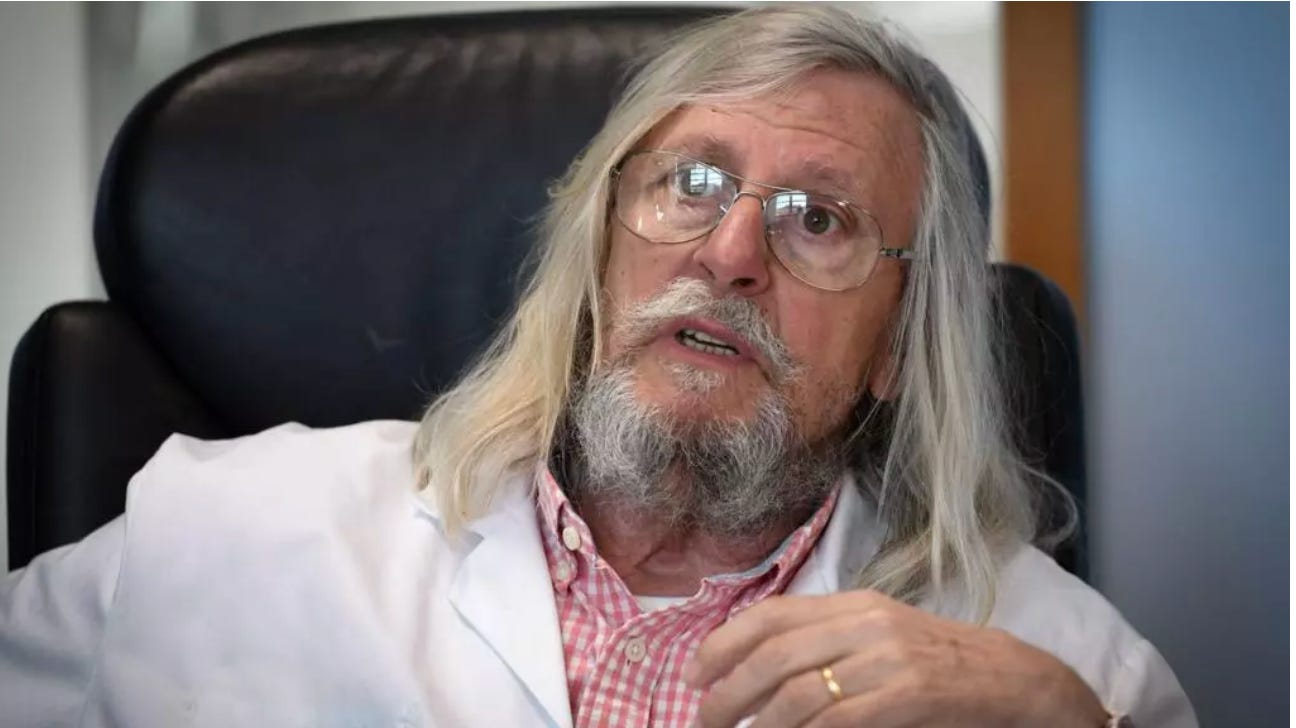
CHAPTER 3: Gandalf of Marseille
Professor Didier Raoult is sometimes referred to in the French press as “Gandalf of Marseille” because of his resemblance to the famous wizard in The Lord of the Rings. The 68-year-old’s appearance—tall, powerfully built, with shoulder length hair and white mustache and goatee—expresses his larger-than-life character and biography. Others have opined that he looks like a medieval knight in a white lab coat. Still others have likened him to Panoramix the Druid in the Asterix comic series about a village of Gauls who resist Julius Caesar’s Roman occupation. The latter comparison is apt, because one of Professor Raoult’s most conspicuous traits is his indomitable spirit of independence.
Born in 1952, Didier Raoult spent his early years in Dakar, French West Africa (now Senegal) where his father, a military doctor with the rank of colonel, was posted. Malaria was endemic to the region, so he and his family took hydroxychloroquine as a prophylaxis. In 1961 his family moved back to Marseille. He briefly attended high school in Nice and Briancon, and then dropped out to join the French merchant marine, where he worked on a ship called the Renaissance. Again, returning to Marseille, he studied literature for a year, and then switched to medicine. He earned his MD and then a PhD in biology.
It’s tempting to think he was destined to be an infectious disease researcher, achieving international renown reminiscent of Louis Pasteur’s. His father, Dr. Andre Raoult, was head of a commission in French West Africa to investigate the main causes of death in the territory. His maternal great, great grandfather, Louis Paul Le Gendre, was also a doctor and infectious disease researcher who published 260 academic papers and chaired the French Society for the History of Medicine. Following in the footsteps of his distinguished ancestors, Dr. Raoult made the research and treatment of infectious diseases his life’s calling. A May 12, 2020 feature in the New York Times introduced him to American readers as follows:
Raoult ... has made a great career assailing orthodoxy, in both word and practice. “There’s nothing I like more than blowing up a theory that’s been so nicely established,” he once said. He has a reputation for bluster but also for a certain creativity. He looks where no one else cares to, with methods no one else is using, and finds things.
A tireless researcher, he has published 2,300 papers and is the most cited microbiologist in Europe. He and his team have discovered 468 species of bacteria—about 1/5 of all those named and described. The bacteria genus Raoultella was named in his honor. He is probably best known as the discoverer of the so-called giant virus, so large it had previously been mistaken for an intracellular bacterium. He has won 13 major awards and is a Commander of the National Order of Merit.
In 2010 he was instrumental in founding a group of university research hospitals (IHUs)—including his own in Marseille, called the Institut Hospitalo-Universitaire Méditerranée Infection. These IHUs were established as foundations with access to private donations and independence from the state. Though the French state has frequently honored him for his achievements (he is a member of the Legion of Honor) in recent years he’d clashed with heads of national medical institutions.
Especially tense has been his relationship with Dr. Yves Levy, who served as Director of the National Institute of Health and Research from 2014-2018. An immunologist, Dr. Levy spent his formative years researching HIV, seeking an elusive vaccine against the virus, and working in various research units of the National Institute of Health. Dr. Levy was also part of the French delegation that inaugurated the BSL-4 Lab at the Wuhan Institute of Virology in 2017. The lab was conceived in 2003 during the SARS-CoV-1 outbreak and constructed by the French biotech company bioMerieux SA pursuant to a cooperative agreement between France and China. The CEO of bioMerieux from 2007-2011 was Stephane Bancel. In 2011 it seemed like an extraordinary—perhaps even Quixotic— decision to leave this plum position to become the CEO of the small, Cambridge, Massachusetts startup Moderna. At the time, the company had one employee and was exclusively focused on developing mRNA therapeutics.
“When I resigned from my last company, bioMerieux, to start on this journey at Moderna, I told my wife there was only a 5% chance it would work out,” Bancel stated in a December 2020 interview.
In many respects, Dr. Yves Levy’s career paralleled that of Dr. Anthony Fauci—Director of the National Institute of Allergy and Infectious Diseases (NIAID) in the United States, who also devoted many of his formative years to HIV research and vaccine development. In 2016, Drs. Levy and Fauci were appointed members of the UN’s Global Health Crisis Task Force. According to Professor Raoult, who stated his opinion to the French press that “the pursuit of a vaccine for HIV is a fantasy that has cost billions and will never be realized.”
This remark and others about the National Institute of Health—spoken with Professor Raoult’s characteristic lack of diplomacy—did not endear him to Dr. Levy. Their long simmering “reciprocal detestation” erupted into open conflict in 2017, when Director Levy’s wife, Agnès Buzyn, became the French Minister of Health. Shortly thereafter she attempted to change the foundation status of IHUs to that of public interest groups under the executive direction of the National Institute of Health. Professor Raoult cried foul and accused Minister Buzyn of pursing policy in the interest of her husband, and not in the interest of medical science.
“The IHUs are an issue of authority and territory for Yves Lévy. He would like to lead them from Paris,” Professor Raoul declared to the French weekly newsmagazine, Marianne. “Yves Lévy gave orders to everyone; he believes he can make us obey. Great scientists do not obey anyone.”
In the end, Professor Raoult prevailed and IHUs retained their original legal status. Professor Levy’s tenure at the National Institute of Health concluded in 2018, but his wife remained the Minister of Health, where she was serving in 2020 when COVID-19 arrived in France.
As a treating physician and researcher, Professor Raoult had long been interested in drug repurposing—that is, experimenting with existing medicines, already approved for treating some diseases, to determine if they are useful for treating others. As the New York Times profile put it:
Hundreds and hundreds of molecules have already been approved for human use by the Food and Drug Administration. Hidden among these, Raoult contends, are various unanticipated cures. “You test everything. ... You stop pondering; you just look and see if, by chance, something works. And what you find by chance, it’ll knock you on your derrière.”
For decades he’d been interested in the anti-microbial properties of hydroxychloroquine. Though the drug was originally developed to prevent and treat malaria, it had proven to have an array of a salutary effects. In the 1990s, he gave hydroxychloroquine a try against Q fever, an often-deadly disease caused by an intracellular bacterium, which, like viruses, multiply within the host’s cells. Raoult discovered that hydroxychloroquine reduces acidity inside the cells, thereby inhibiting bacterial growth. He commenced treating Q fever with a combination of hydroxychloroquine and doxycycline. Later he used the same combination to treat Whipple’s disease, another frequently fatal condition, also caused by an intracellular bacterium. Professor Raoult’s combination therapy is now widely regarded as the standard treatment for both diseases.
In 2003 he followed the outbreak of SARS-CoV-1 in China and was familiar with the literature on the anti-viral properties of chloroquine and hydroxychloroquine against the novel virus. In 2007 he reviewed the evidence in his own paper and concluded that hydroxychloroquine might be “an interesting weapon to face present and future infectious diseases worldwide.” In 2018, he reported that azithromycin had potent activity in cells infected with Zika virus.
When SARS-CoV-2 broke out in 2020, again emanating from China, he wanted to know how Chinese doctors were treating the disease. In February, he saw reports from multiple Chinese research teams stating that chloroquine and hydroxychloroquine were reducing disease severity and accelerating clearance of the virus. The People’s Hospital of Wuhan University posted a notice on its website that none of the 178 patients admitted so far had lupus, suggesting the hydroxychloroquine they were taking to treat lupus may have prophylaxis value against COVID-19. On February 19, a pharmacology research team in Qingdao, China published a report in English that on February 17, the State Council of China held a news briefing in which it announced that chloroquine phosphate had demonstrated marked efficacy and acceptable safety in treating COVID-19. After positive in vitro studies, several clinical trials were conducted to test chloroquine and hydroxychloroquine for the treatment of COVID-19.
Thus far, results from more than 100 patients have demonstrated that chloroquine phosphate is superior to the control treatment in inhibiting the exacerbation of pneumonia, improving lung imaging findings, promoting a virus-negative conversion, and shortening the disease course, according to the news briefing. ... Given these findings ... the drug is recommended for inclusion in the next version of the Guidelines ... issued by the National Health Commission of the People’s Republic of China.
For Professor Raoult, this report was cause for jubilation. Facing a pandemic that could inflict untold suffering and death on mankind, it appeared that a well-known, safe, cheap, and easy to manufacture drug was effective at treating it. Wanting to share this good news, on February 25 he posted a video on YouTube titled Coronavirus: Game Over!
“It’s excellent news — this is probably the easiest respiratory infection to treat of all,” Raoult said.
He then formulated his own treatment protocol. He chose hydroxychloroquine because it is less toxic than its analogue chloroquine. He combined it with azithromycin because of the anti-viral effect he’d observed in using it against the Zika virus, and for its value against secondary bacterial infections. As for the safety profile of these drugs, they’d been around for decades, with billions of doses taken and well- tolerated. Both hydroxychloroquine and azithromycin are on the World Health Organization’s Model List of Essential Medicines.
At the beginning of March, Professor Raoult announced that he would test and treat anyone who came to his hospital. Come they did, lining up at the entrance. In order to handle the surge, he and his staff erected field tents outside to examine sick patients and give them the combination therapy.
He then briskly performed a clinical study to evaluate the effect of hydroxychloroquine on respiratory viral loads. Presence and absence of the virus at Day 6 post inclusion was the end point. Fourteen were treated with hydroxychloroquine and six were treated with a combination of hydroxychloroquine and azithromycin. The control group was composed of 16 untreated patients from another center and cases refusing the protocol. On Day 6 of the trial, 14 of the 16 control patients still tested positive for the virus. Only 6 of the 14 patients receiving hydroxychloroquine tested positive on Day 6. All 6 patients treated with a combination of hydroxychloroquine and azithromycin had cleared the virus.
Professor Raoult understood the results were not proof of the drug’s efficacy in treating COVID-19. Nevertheless, the study indicated that the cocktail of hydroxychloroquine + azithromycin substantially reduced viral load in the upper respiratory tract. This provided a strong rationale for using it to treat people while performing additional case studies to examine its efficacy. Thus, Professor Raoult quickly published the results of this study in the International Journal of Antimicrobial Agents.
The academic medical community’s response was conspicuously tepid, perhaps even hostile. Given the apparent direness of the situation facing mankind, one might have expected at least an openness to Professor Raoult’s results.
The psychiatrist and author, Dr. Norman Doidge, pointed out that the response was a conspicuous example of “unwishful thinking.” Normal people with no unstated agenda could only wish for a cheap generic drug with an excellent safety profile that could save millions of lives. Conversely, those guilty of unwishful thinking dismissed hydroxychloroquine’s potential benefit even before it had been examined.
Shortly before Professor Raoult’s study was published, he shared it with two independent researchers in the United States, an ophthalmologist named Dr. James Todaro at the Beaumont Hospital in Dearborn, Michigan and a lawyer named Gregory Rigano. They too had seen the Chinese reports, and they’d also seen a February 13 report in the Korea Biomedical Review headlined “Physicians work out treatment guidelines for coronavirus.”
The COVID-19 Central Clinical Task Force, composed of physicians and experts treating the confirmed patients across the nation, held the sixth video conference and agreed on these and other treatment principles for patients with COVID-19. ... if patients are old or have underlying conditions with serious symptoms, physicians should consider an antiviral treatment. If they decide to use the antiviral therapy, they should start the administration as soon as possible. ... As chloroquine is not available in Korea, doctors could consider hydroxychloroquine 400mg orally per day, they said.
On March 13, Todaro and Rigano published their own paper on Google Docs in which they presented the results of the South Korean and Chinese studies recommending chloroquine and hydroxychloroquine for treating COVID-19.23 On March 16, Elon Musk retweeted a reference and link to this paper, thereby rapidly publicizing it.24
On March 19, Rigano went on Fox New’s Tucker Carlson Tonight to talk about Professor Raoult’s study of hydroxychloroquine, claiming it showed “a 100% cure rate.” He concluded by stating that the study was scheduled to appear the next day in The International Journal of Antimicrobial Agents, so viewers could see it for themselves.
Because Rigano was not affiliated with a major academic medical institution and didn’t work for a federal health agency, he lacked medical authority. Mainstream media pundits proclaimed it was absurd for a lawyer to be presenting possible COVID-19 treatments. And yet, the paper that he co-authored with Dr. Todaro was a perfectly competent presentation of the South Korean and Chinese studies, and when he appeared on Tucker Carlson, it was to convey the results of a study conducted by the most cited microbiologist in Europe. Why was the American mainstream media, apart from Fox News, hostile to Rigano’s March 13th paper (co-authored with Dr. Todaro) and his good news about Professor Raoult’s study on March 19?
The South Korean, Chinese, and French studies were not final proof of the efficacy of chloroquine and hydroxychloroquine in treating COVID-19, but they offered hope and a start for further research. That they were instantly shot down suggested that the legacy media did not want these drugs to be useful in treating the disease.
Instead of deriding Rigano and Todaro for their lack of authority, the legacy media should have asked why U.S. federal agencies weren’t talking about the South Korean, Chinese, and French studies. Why weren’t they, and what treatment possibilities were they talking about?
Author’s Note: If you found the above chapter interesting, you will enjoy the entire book The Courage to Face COVID-19: Preventing Hospitalization and Death While Battling the Bio-Pharmaceutical Complex, by John Leake & Peter A. McCullough, MD.
If you look at Wikipedia he is still being attacked and destroyed for being correct. This is so tragic. And everyone suffers from this persecution of a man who thinks out of the box, has curiosity, and understands connections
In Ireland the President of the Irish Medical Council admitted 'everyone was denied this treatment' : (hydroxychloroquine)
https://louiseroseingrave.substack.com/p/former-imc-president-admits-everybody?utm_source=share&utm_medium=android&r=gpx4d