

Situational Update: 2026 UK Outbreak of Neisseria meningitidis, serogroup B (MenB)
30 total (suspected+confirmed) cases, confirmed case fatality rate 10%

By Peter A. McCullough, MD, MPH
The United Kingdom is loaded with expertise and laboratory facilities studying Neisseria meningitidis group B (MenB). Major research and reference laboratories in the UK working with live, pathogenic MenB include specialized university groups and national public health facilities. Research involving live pathogens typically occurs in high containment (Biosafety Level 2 or 3) facilities.
National Public Health & Reference Labs
These facilities provide the UK’s primary diagnostic and surveillance capabilities for live MenB strains.
Meningococcal Reference Unit (MRU), UKHSA (Manchester): Located at Manchester Royal Infirmary, the Meningococcal Reference Unit provides confirmatory laboratory services and genetic analysis for meningococcal disease outbreaks across England.
National Institute for Biological Standards and Control (NIBSC): Based in South Mimms, the NIBSC plays a critical role in developing serum standards and testing the efficacy of MenB vaccines like Bexsero.
Leading University Research Labs Working with Strains of Meningitis Serotype B
The following academic institutions maintain active research portfolios focused on MenB pathogenesis, carriage, and vaccine development.
Oxford Vaccine Group (University of Oxford): A global leader in meningococcal research, the Oxford Vaccine Group recently developed the ChAdOx1 MenB (using a replication-deficient adenoviral vector) vaccine candidate and conducts extensive studies on MenB carriage in teenagers.
Tang Lab, Sir William Dunn School of Pathology (University of Oxford): This lab focuses on the molecular basis of infection and recently collaborated with the Serum Institute of India to develop a new protein-based MenB vaccine.
Maiden Lab (University of Oxford): Specializes in the population biology and genomics of N. meningitidis, using whole-genome sequencing to track MenB strains.
Spencer Dayman Meningitis Laboratories (University of Bristol): This facility stores and analyzes tens of thousands of samples to study meningococcal disease and carriage among UK students.
Vaccine Institute, St George’s (University of London): Conducts clinical trials and laboratory research specifically on Meningococcus B to improve vaccine schedules for infants.
Imperial College London: Researchers at the MRC Centre for Global Infectious Disease Analysis perform modeling and laboratory analysis on the impact of MenB vaccination.
Alter AI aided in this concise epidemiological briefing for the 2026 Kent MenB outbreak (”Kent strain” (ST-41/44 complex).
🧠 Overview
Pathogen: Neisseria meningitidis, serogroup B (MenB)
Clinical syndrome: Invasive meningococcal disease → meningitis / septicaemia
Under UKHSA guidance, a clinical diagnosis of meningitis implies:
Fever > 38 °C,
Neck stiffness or positive Kernig/Brudzinski signs,
Altered sensorium or photophobia, and —
CSF pleocytosis (elevated white blood cells), or, if CSF unavailable, a clinician’s diagnosis of meningitis prompting parenteral antibiotics.
If N. meningitidis is detected by culture or PCR → Confirmed MenB subtype
Hospital care: IV ceftriaxone or cefotaxime, IV dexamethasone, supportive care
Index location: Club Chemistry nightclub, Canterbury (5–7 Mar 2026)
Epicentre: University of Kent Canterbury Campus + East Kent Schools
Declaration: UKHSA regional outbreak 13 Mar; national alert 15 Mar 2026
Declared “super‑spreader event” by UKHSA Chief Exec Susan Hopkins
📊 Epidemiological data
Total Cases=30 (20 laboratory‑confirmed MenB; 9 probable) Hospitalised=26, Deaths=2 (University student 21 M + School pupil 18 F, both MenB confirmed) Active critical cases 5 (ICU; 2 induced comas). Linked sites University of Kent, CCC University, 7 secondary schools (Faversham, Ashford, Broadstairs) UK counties affected Kent (primary), London (1 case, Kent resident), Paris region (1 exported case, exchange student from Kent). Suspected case as of March 20, 2026, St John Rigby College in Orrell, Wigan (near Manchester) visited Kent the week previous week. Average age affected 17–22 yrs (adolescents and young adults) Estimated fatality rate so far ~ 10.0 % (2 / 20 confirmed) — typical for MenB Hospital stay median 6 days (3–10 range noted) Symptom to hospital window ≈ 48–72 hours (rapid progression pattern)

🧩 Key Determinants & Transmission
Primary exposure: Crowded nightclub contacts at Club Chemistry (Canterbury).
Secondary clusters: University halls of residence and school social events.
Mode: Respiratory droplet / saliva via close contact (kissing, talking close face to face).
Incubation: 3–5 days.
Super‑spreader factors: Confined indoor space, recycled air flows, shared drinking and smoking vessels.
🧬 Public Health Actions
Antibiotic prophylaxis: > 6,500 doses given (Ciprofloxacin single 500-750 mg dose for carrier eradication).
Vaccination drive: Targeted MenB programme dose 1, then dose 2 at 30 days, then protection begins ~2 weeks after second dose. It was given to ≈ 5,000 University of Kent students in halls. Because MenB bacteria are highly diverse, the vaccine's effectiveness depends on whether the outbreak strain expresses the antigens included in the vaccine (fHBP, NadA, NHBA, and PorA P1.4).
Closures: Club Chemistry (indefinite); Simon Langton & other schools Year 13 temporarily closed.
Testing: PCR confirmation via East Kent Hospitals University NHS Foundation Trust.
Contact‑tracing: ≈ 30,000 students + families notified.
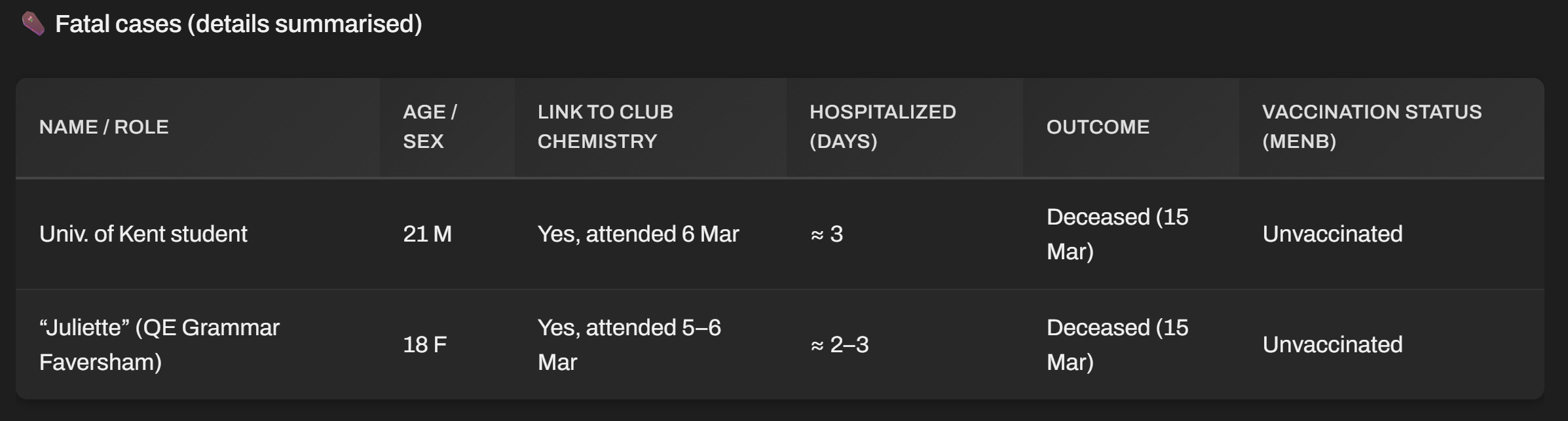
⚰️ Fatal cases (details summarised)
🚨 Critical Observations
Vaccine gap: All victims born before 2015 → no public MenB coverage under NHS schedule, however parents may have vaccinated them by private pay and NHS is not revealing vaccine status.
Systemic oversight: Delay (≈ 24 h) between first hospital notifications and UKHSA public alert; criticized by MP Helen Whately and The Times.
Possible policy shift: MenB catch‑up programme for teens now under urgent HHS review.
🔍 Interpretive Note
The Kent cluster demonstrates how a single mass indoor event can initiate a cluster of serious cases among likely unvaccinated young persons. In adults, high antibody levels typically persist for several years after vaccination, though they do decline over time. Unlike some other vaccines, Bexsero does not provide “herd immunity” (it doesn’t reliably stop the bacteria from living in the throat), so it provides partial protection to the individual who is vaccinated. Continued transparency in vaccine status data will determine the credibility of UKHSA and NHS responses to future bacterial outbreaks.
Please subscribe to FOCAL POINTS as a paying ($5 monthly) or founder member so we can continue to bring you the truth.
Peter A. McCullough, MD, MPH
President, McCullough Foundation
FOCAL POINTS has partnered with Patriot Mobile to defend your medical freedom. Join Patriot Mobile today!

"If N. meningitidis is detected by culture or PCR → Confirmed MenB subtype"
PCR doesn't I.D. a particular virus, according to the PCR inventor, Kerry Mullis.... who "died suddenly" in the fall of 2019... the fall where event 201 took place for the plandemic planning.
Can't believe any of this nonsense, if the PCR is the method of detection.
Why would Dr. McCullough, play this game?
If we took 10,000 or 100,000 people in a population how many carry this bacteria ? Why does it suddenly appear ? Is it that those affected lack something in their immune systems ?