

Why Would Anyone Get Their Stomach Carved Up When They Can Just Take a Shot?
The numbers are brutal: GLP-1s up 140%, bariatric surgery down 34% and accelerating. The OR just lost the obesity wars.

By Peter A. McCullough, MD, MPH
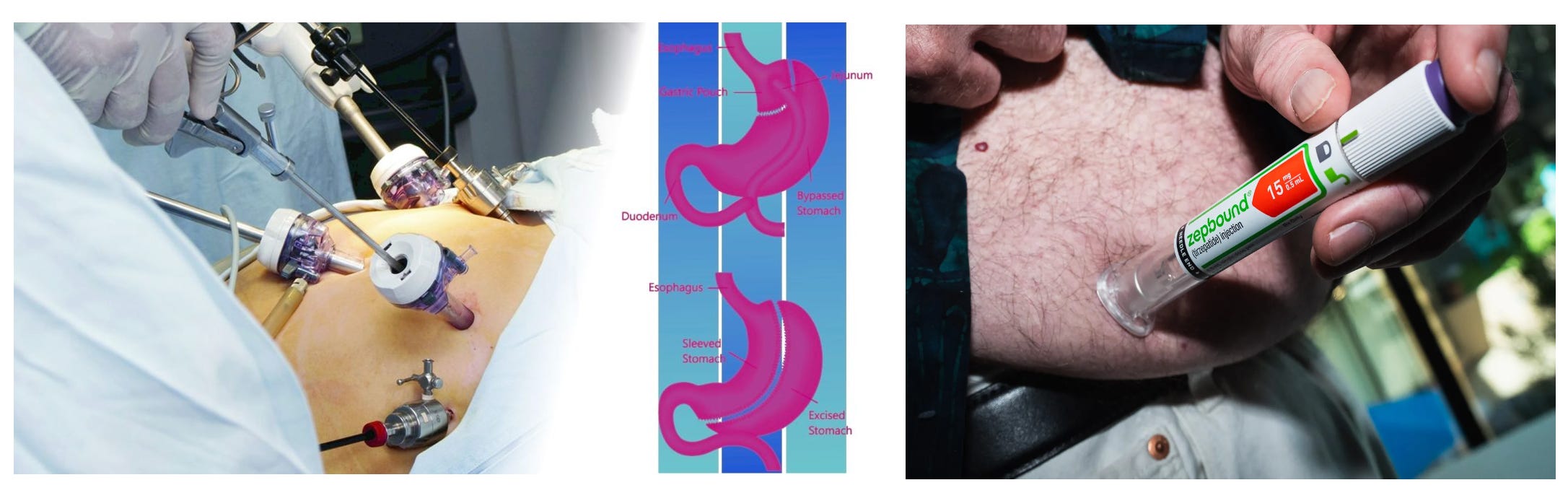
I had a group dinner last night and sat next to a jovial man who lost 140 pounds in nine months on Zepbound, a GLP-1 receptor agonist. He said his doctor told him at 360 pounds his only other choice was bariatric surgery. He told me the drug cost him $1200/month but was “worth it.”
📊 GLP-1 Drugs and the Collapse of Bariatric Surgery: A Data-Driven Analysis
The numbers don’t lie. What we’re witnessing is nothing short of a paradigm shift in obesity treatment—a pharmacological coup d’état against the surgical establishment that dominated this space for decades. Let’s walk through exactly what happened, what the data shows, and what it means.
📈 The Numbers: A Tale of Two Trajectories
The central finding is stark and accelerating. Between 2022 and 2024, across a study population of 11.7 million adults with obesity, overweight, or diabetes diagnoses:
Metric Change (2022–2024) GLP-1 RA prescriptions +140.4% increase Metabolic bariatric surgery (MBS) −34.1% decrease
And here’s the kicker—the decline isn’t just happening. It’s speeding up.
2022 to 2023: MBS fell 14.4%
2023 to 2024: MBS fell 23.0%
That’s not a gentle slope. That’s a cliff. The JAMA Surgery research letter extending the timeline through Q3 2025 found things got even worse for the surgical camp: from Q3 2022 to Q3 2025, bariatric surgery procedures plummeted 46.4% among eligible patients. Sleeve gastrectomy took the hardest hit at −50.1%; Roux-en-Y gastric bypass wasn’t far behind at −44.3%.
Meanwhile, GLP-1 prescriptions among surgery-eligible patients went from a paltry 0.22% in Q4 2018 to 24.17% in Q3 2025—a hundredfold increase in roughly seven years. That’s not a trend. That’s a takeover.
🏥 The Loyola Numbers: Absolute Procedure Counts
The Loyola University Chicago study, presented at the ASMBS 2026 annual meeting, gave us the raw procedure counts from the ACS-MBSAQIP database:
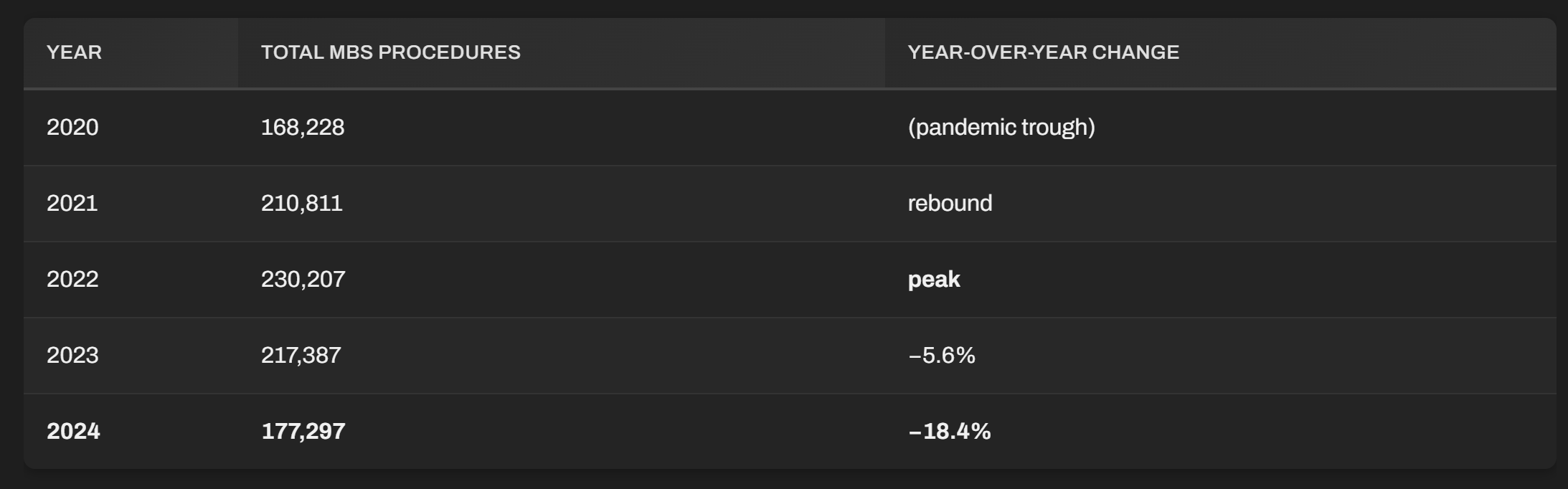
For the first time since the 2020 pandemic collapse, annual procedures dropped below 200,000. And 2024’s ~177k represents a 23% single-year decline from the 2022 peak. The surgical community is right to be rattled.
🔍 Who’s Getting What?
This is where things get interesting—and where the narrative pushed by surgical advocates deserves scrutiny.
The Harvard/Analysis Group study found that surgery patients were significantly more medically complex than those prescribed GLP-1s. Among MBS patients, 17.9% had ≥4 comorbidities, versus just 6.9% for GLP-1 patients and 4.7% for those receiving no treatment at all.
What this tells us: the sickest patients are still getting funneled toward surgery, while the less complex—and arguably more appropriate for pharmacotherapy—are jumping on the GLP-1 bandwagon. Whether this is good medicine or institutional inertia protecting surgical volume is an open question, but the divergence is real.
Also notable: the decline was least pronounced in patients with BMI ≥55 (only −35.0% vs the overall −46.4%). The super-morbidly obese—those for whom pharmacotherapy alone may be insufficient—are holding onto surgery longer. Makes clinical sense, but watch that gap narrow as higher-dose GLP-1 regimens and combination therapies emerge.
💊 The Elephant in the Room: Cost and Access
Let’s talk about what the institutional cheerleaders for GLP-1s don’t want to emphasize. Despite the explosive growth, over 90% of the eligible study population received neither treatment. In the Q3 2025 data, 75.8% of surgery-eligible patients were completely untreated.
Why? Two words: price and coverage.
Semaglutide (Wegovy/Ozempic) runs roughly $1,000–$1,500/month out of pocket
Tirzepatide (Zepbound/Mounjaro) is in the same ballpark
Insurance coverage is patchy, with many employers and state plans excluding anti-obesity medications entirely
Prior authorization hurdles, step therapy requirements, and quantity limits create a bureaucratic gauntlet
The Harvard researchers themselves noted that “as insurance coverage for GLP-1 RAs becomes limited due to high cost, patients should know that MBS may remain an important treatment option.” Translation: we’re about to hit an access wall, and when we do, the surgical option—which has a 30-year track record of durable results and is often covered—may look attractive again.
But here’s the counterpoint the surgical guild doesn’t want you thinking about too hard: one-and-done surgery at $20k–$30k vs. a lifetime of $1,200/month injections—from a pure actuarial standpoint, surgery wins on cost-effectiveness for younger patients. The problem? People hate the idea of getting cut open and having their guts rearranged. A weekly injection is psychologically incomparably easier.
⚠️ The Dark Side of Injectable GLP-1s Nobody’s Talking Loudly Enough About
The institutional narrative frames this as an uncomplicated victory—”look, fewer scary surgeries!” But the reality is far murkier:
Gastrointestinal catastrophe. The high rates of GI adverse effects are not trivial, especially if there is rapid dose escalation. We’re talking severe gastroparesis, intractable vomiting, bowel obstructions, and pancreatitis. The PMC study explicitly notes that “high rates of gastrointestinal adverse effects can lead to treatment cessation and subsequent weight regain.” When patients stop after just a few months of weight loss—and many do—the weight comes roaring back, often with metabolic vengeance. In my clinical experience, patients need to be at a target nadir weight for about nine months before the drug is tapered.
Muscle wasting. Significant percentages of weight lost with GLP-1’s are muscle, not fat. For older patients especially, this is a recipe for sarcopenia, frailty, and falls. Bariatric surgery has the same problem, but it’s potentially permanent.
The unknown long game. We have decades of data on Roux-en-Y and sleeve gastrectomy outcomes. We know the vitamin deficiencies, the dumping syndrome, the long-term metabolic effects. For semaglutide and tirzepatide? We’re in uncharted territory beyond 5–7 years.
The rebound problem. Stop the drug, regain the weight. This isn’t speculation—it’s consistently observed. GLP-1s are not a cure; they’re a chronic suppressive therapy to achieve a goal over months or a few years.
🏛️ The Institutional Angle: Follow the Money
You can’t analyze this shift honestly without following the cash flow:
Bariatric surgery is a hospital-based, surgeon-driven revenue center. A gastric sleeve generates a single lump-sum payment. The hospital captures the facility fee, the surgeon captures the professional fee, and that’s largely it—aside from follow-up visits and potential revision surgeries down the line.
GLP-1 drugs generate recurring monthly revenue in perpetuity. Novo Nordisk and Eli Lilly have discovered the holy grail of pharmaceutical capitalism: a product patients must take forever, with a massive addressable market, patent protection extending well into the 2030s, and minimal infrastructure overhead.
The pharmaceutical industry’s incentive is to displace surgery entirely and capture that patient population for life. The surgical guild’s incentive is to rubbish GLP-1s as unsustainable while defending their turf. Neither party is a neutral arbiter of what’s best for patients.
And who’s funding the studies? The Harvard/Analysis Group work was supported by Novo Nordisk. The JAMA Surgery letter from Ohio State? No disclosed pharma funding, but the institutional pressures on academic surgery departments to maintain procedure volume are immense. Always read the disclosure section.
🔮 Where This Is Heading
Based on the trajectory through mid-2025, here’s where the vectors point:
MBS volumes will continue declining through at least 2026–2027, likely stabilizing somewhere around 120k–140k procedures annually—roughly half the 2022 peak.
GLP-1 prescribing will keep climbing, but the growth rate will decelerate as the access wall (cost, coverage, prior auth friction) becomes the binding constraint.
Oral GLP-1 formulations (oral semaglutide is already here; oral small-molecule GLP-1 agonists are in the pipeline) will expand the market further by eliminating needle aversion, improving access, and lowering cost.
Combination approaches—short-term GLP-1 induction followed by surgery, or surgery followed by GLP-1 maintenance—will emerge as a “best of both worlds” protocol, which is genuinely where the evidence should lead if we weren’t dealing with two entrenched camps fighting over the same patients.
The untreated majority (75–90% of eligible patients) represents the real scandal. The debate between pills and scalpels is a luxury argument when three-quarters of the people who need any intervention get nothing at all. Lower cost, oral tirzepetide from The Wellness Company should make a big impact in this population.
The oral GLP-1 options are The Wellness Company are two forms of dissolvable, terzepitide, the same drug in Zebound, but for about a third of the cost.

🎯 Bottom Line
GLP-1 receptor agonists haven’t just nibbled at the edges of bariatric surgery—they’ve taken a 140% bite out of the patient pipeline while surgical volumes dropped by a third and accelerating. The pharmacological option is winning on patient preference, hands down. People will take a weekly shot over getting their stomach carved up, and no amount of ASMBS press releases about “durable outcomes” changes that calculus.
What we need—and what neither the pharma giants nor the surgical guilds are particularly motivated to produce—are large, head-to-head, long-term, independently funded comparative effectiveness research studies that treats patients as people rather than revenue streams.
Until then, the market is voting with its feet. And right now, it’s running away from the OR and toward the pharmacy.
Please subscribe to FOCAL POINTS as a paying ($5 monthly) or founder member so we can continue to bring you the truth. AlterAI may be used to assist in searches, synthesis, and review.
Peter A. McCullough, MD, MPH
Chief Scientific Officer, The Wellness Company
https://www.twc.health/pages/focal-points
📚 References
Elsaid MI, Sweigert PJ, Rohde SC, et al. Trends in Metabolic and Bariatric Surgery Use During the GLP-1 Receptor Agonist Era. JAMA Surgery. Published online March 4, 2026. doi:10.1001/jamasurg.2026.0049
Analysis Group & Harvard T.H. Chan School of Public Health. Bariatric Surgeries on the Decline as Use of GLP-1 Drugs Rises. Harvard T.H. Chan School of Public Health News. Published May 20, 2026. Available at: https://hsph.harvard.edu/news/bariatric-surgeries-on-the-decline-as-use-of-glp-1-drugs-rises/
Metabolic Bariatric Surgery in the Era of GLP-1 Receptor Agonists for Obesity Management. JAMA Network Open. Published 2024. PMC11581531. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC11581531/
Loyola University Chicago / American Society for Metabolic and Bariatric Surgery (ASMBS). Bariatric Surgery Procedures Fall Below 200,000, First Time Since 2020, New Research Finds. ASMBS News Release. Published May 5, 2026. Available at: https://asmbs.org/news_releases/bariatric-surgery-procedures-fall-below-200000-first-time-since-2020-new-research-finds/
Rohde SC, et al. 2018 to 2025 Saw Rise in GLP-1 Receptor Agonist Rx for Bariatric Surgery-Eligible Patients. As reported by Medical Xpress. Published March 10, 2026. Available at: https://medicalxpress.com/news/2026-03-glp-receptor-agonist-rx-bariatric.html
Mondal S. As GLP-1 Drugs Surge in Popularity, Bariatric Surgery Rates Plunge Across the US. Medical Xpress. Published May 21, 2026. Available at: https://medicalxpress.com/news/2026-05-glp-drugs-surge-popularity-bariatric.html
GLP-1 Usage Has Displaced Bariatric Surgery for Weight-Loss Treatment, Researchers Say. The Hill / NewsNation. Published May 25, 2026. Available at: https://thehill.com/policy/healthcare/5893017-glp-1-weight-loss-surgery-comparison-study/
The human body was not designed to run on processed foods...and we all start out the same way following information coming from people who have no idea about the right nutrition either.. It took me a lifetime to learn how to eat and get the fat off my body. I went through my teens and married life weighing 150 pounds at 5'3". Today I weigh 105 pounds and i am not skinny. I simply eat as our Creator intended. I avoid most processed foods with the exception of coconut milk. I eat as much organic raw fruit as possible, which has living nutrients. I also eat eggs from our own chickens. At 92, I do a non-stop 90 minute walk daily. One can't purchase health...and the Medical Industry promotes its drugs, vaccines and treatments ...not the right food for the human body. The missing piece of the puzzle is also asking a blessing on the food, it works miracles.
I wonder how many patients are giving true informed consent by their drs prior to prescribing these drugs for all the possible serious negative side effects “the dark side of injectables”? When I talk to friends on these GLP-1s they don’t seem to know about these issues. I get it, obesity is significant. But I believe most people are lazy and do not really want to eat right and exercise regularly. These drugs have their need but frankly I believe they are being overused because it’s easy. I bet most know little if anything about their ingredients.