

1916 New York Polio Epidemic: Lab Leak from Rockefeller Institute?
The unique and virulent epidemic that erupted in Brooklyn in May-June 1916 has long been a fascinating mystery. A 2011 paper presents a plausible solution.

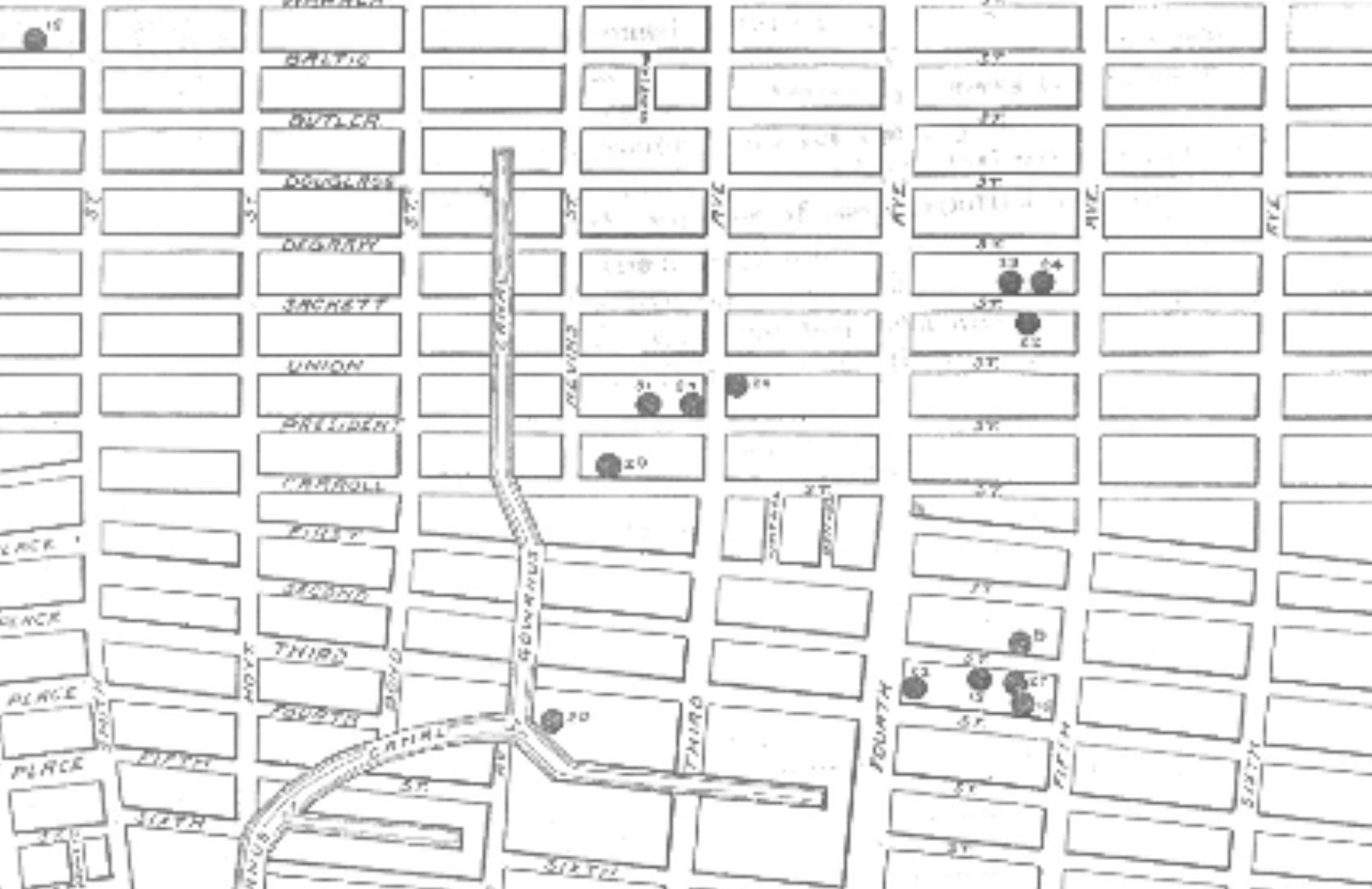
Last year, when I was researching polio for our book Vaccines: Mythology, Ideology, and Reality, I was struck by the uniqueness of a 1916 epidemic of paralytic polio in New York City. The disease broke out in what was then a poor neighborhood of Brooklyn, largely inhabited by recently arrived Italian immigrants. The area was characterized by overcrowding and unsanitary conditions. The Gowanus Canal, near the outbreak epicenter, was severely contaminated with raw sewage.
In 1916, Brooklyn was in the process of getting hooked up to city water piped from clean Catskill reservoirs. However, it seems that many residents in poor areas were still drawing water from municipal or private wells that were vulnerable to ground water contamination.
What caught my eye about the 1916 Brooklyn epidemic was that it behaved and spread much like the Soho (London) cholera epidemic in 1854 (documented by Dr. John Snow) and a major diphtheria outbreak in the Montparnasse neighborhood of Paris in the mid 1880s, chronicled by Dr. Axel Munthe in his memoirs, The Story of San Michele.
Though the causative agents were different, each of these infectious disease epidemics was traced to an outbreak epicenter from which cases of severe illness radiated outward in a distinct spread pattern.
The following images display the Brooklyn epicenter of the 1916 polio epidemic.
To appreciate the peculiarity of the 1916 outbreak, it is important to understand the peculiar nature of polio. As we note in our book, Vaccines: Mythology, Ideology, and Reality:
During the 1940s and early ’50s, with the incidence of all other infectious diseases having dramatically decreased, increasing attention was focused on poliomyelitis, commonly known as polio. Poliomyelitis comes from the Greek words polios (grey), meulos (marrow) and itis (inflammation)—that is, inflammation of the gray matter of the spine. According to the CDC, about 75 percent of people infected with poliovirus experience no symptoms, while about 25 percent experience mild or flu-like symptoms that may be mistaken for many other illnesses. Approximately 1 out of 200 people to 1 in 2000 people, depending on virus type, experience paralysis or weakness in the arms, legs, or both.[i]
Only humans suffer from polio disease, though Chimpanzees and Old-World monkeys can be experimentally infected with the virus, which grows well in monkey kidneys. The infection is thought to have been endemic to all human populations since ancient times. According to conventional history, the first modern medical reference to the disease was in the 1789 A Treatise on Diseases of Children by the English physician Michael Underwood, who described it as a “debility of the lower extremities in children.” The book makes no reference to outbreaks of the disease. The first detailed clinical description was written by the German orthopedic doctor, Jakob Heine, in 1840.
In 1909, the Austrian physicians Karl Landsteiner and Erwin Popper hypothesized that polio may be caused by a “virus” in the modern sense of the word—this is, submicroscopic infectious agent.[ii]
With increasing urbanization in Europe and America between 1650-1950, it’s likely that everyone was exposed to the poliovirus during infancy and early childhood, but the medical literature records no notable clusters of paralytic polio before 1894, when an outbreak in Vermont was documented. The disease only became a serious public health problem at the beginning of the 20th century, when communities in the United States experienced what may be characterized as epidemic outbreaks, especially during the summer months. This was likely an unforeseen consequence of hygiene and sanitation improvements at the turn of the 20th century, which resulted in larger numbers of infants ceasing to encounter the pathogen during their early childhood years, between the ages of six months and five years, when the disease is typically very mild and confined to the throat and GI tract.[iii] Likewise, and increasing number of girls did not encounter the pathogen before they began bearing children, and therefore did not pass maternal immunity to to their nursing infants, thereby protecting them during the first six months of life.
The lack of exposure to polio at a young age was apparently more common among the affluent, making them more vulnerable to severe disease later in life. A notable patrician who was thought to have been struck by paralytic polio—at the age of thirty-nine—was Franklin Delano Roosevelt in the summer of 1921. Roosevelt’s paralysis and struggle to recover ultimately came to be known by the public as a notorious case of polio, though the diagnosis was never laboratory confirmed, and it’s possible he was struck by another illness such as Guillain-Barré syndrome.[iv]
The 1916 epidemic of paralytic polio in New York—which was exceptionally virulent—is mysterious because it happened in a poor, unsanitary neighborhood in which most of the victims had almost certainly been exposed to wild strains of polio in previous years.
Though it is tempting to think that recently arrived Italian immigrant children were immunologically naive to polio strains circulating in New York, the outbreak spread to other boroughs and resulted in paralytic cases among native New Yorkers. The distinct epicenter and strikingly uniform, radial spread strongly suggest that a novel and exceptionally virulent strain of an infectious disease pathogen was the cause.
As Dr. Suzanne Humphries and Roman Bystrianyk (Dissolving Illusions)—as well as Forrest Maready (The Moth in the Iron Lung)— have pointed out, there is a vast amount of documentary literature on other possible causes of paralysis and weakness in the legs, including heavy exposure to environmental toxins such as lead arsenate pesticide and DDT.
Other diseases that could be misdiagnosed as polio are Guillain-Barre syndrome, Coxsackievirus, transverse myelitis, and muscular dystrophy.
However, it’s unlikely that any of these other causes of disease and disability was the culprit of the rapidly spreading disease that was observed in New York, starting in Brooklyn, in May and June of 1916. I can find no record of lead arsenate pesticide being used on trees in the Brooklyn neighborhood in 1916, and DDT was not used for mosquito spraying until the late 1930s. Clusters of Guillain-Barre syndrome, transverse myelitis, and muscular dystrophy would not have caused such a distinct pattern of spreading disease.
It is possible that the 1916 epidemic was caused by a virulent strain of the Coxsackievirus (a type of enterovirus), which has been known to cause epidemics of acute flaccid paralysis (AFP) that mimic polio. However, this is a purely hypothetical possibility, as there is no documentary evidence to support it.
All things considered, the most plausible hypothesis is that the 1916 New York epidemic was indeed caused by an exceptionally virulent strain of polio.
For a long time it has seemed to me that ascertaining what exactly caused the 1916 epidemic could greatly enhance our understanding of the general phenomenon of paralytic polio in the 20th century.
This morning, while pondering this fascinating subject, I started poking around online and found a 2011 paper that I somehow missed when I was doing research on polio last year.
The author, Harold V. Wyatt is a British academic and Honorary Lecturer in Philosophy at the University of Leeds. A noted expert in the history of medicine and microbiology, his research has focused on the history of poliomyelitis, epidemics. His paper—The 1916 New York City Epidemic of Poliomyelitis: Where did the Virus Come From?—presents an intriguing hypothesis based on the following observation:
Three miles from the epicentre of the outbreak, Simon Flexner and his associates at the Rockefeller Institute at 63rd Street and York Avenue, near Queensborough Bridge on Manhattan Island, had been passaging spinal cord tissue con- taining poliovirus, from one Rhesus monkey spinal cord to another. They had been unable to infect monkeys by feeding. These experiments continued with the passage virus which at times was reinforced with newly acquired virus from patients. . . .
. . . I suggest that by 1916, mutants of the original Rockefeller virus had been selected for replication in monkey motor neurones, but were still capable of high levels of replication in other cells. An animal-house worker might have been infected during a post-mortem examination, with accidental carriage into a household in Brooklyn and probably further dissemination in the community until it reached susceptible children without immunity. It would have been the same type that caused the 1907 epidemic which had still been circulating. With its passage through many cycles of human guts in the months that followed, it became more adapted to humans and finally lost its unique characteristics.
A few blocks from the Rockefeller Institute at Lexington Avenue and 63rd Street the 3rd Avenue elevated line linked at Municipal Building station to the BRT line to Brooklyn over Brooklyn Bridge with a stop at 3rd Street and 5th Avenue where the first case lived.
Click on the image below to read Professor Wyatt’s paper in full.

[i] About Polio in the United States, CDC, https://www.cdc.gov/polio/about/index.html
[ii] Karl Landsteiner and Erwin Popper. Uebertragung der Poliomyelitis acuta auf Affen [Transmission of Poliomyelitis acuta to monkeys]. Zeitschrift für Immunitätsforschung und experimentelle Therapie [Journal for Research on Immunity and Experimental Therapy], 2 (4): 377–390, 1909. https://babel.hathitrust.org/cgi/pt?id=uc1.b3208372&view=1up&seq=389&skin=2021
[iii] Robertson S. Module 6: Poliomyelitis (PDF). The Immunological Basis for Immunization Series. Geneva, Switzerland: World Health Organization, 1993. https://web.archive.org/web/20110524151308/http://whqlibdoc.who.int/hq/1993/WHO_EPI_GEN_93.16_mod6.pdf
[iv] Goldman AS, Schmalstieg EJ, Dreyer CF, Schmalstieg FC Jr, Goldman DA. Franklin Delano Roosevelt’s (FDR’s) (1882-1945) 1921 neurological disease revisited; the most likely diagnosis remains Guillain-Barré syndrome. J Med Biogr. 2016 Nov;24(4):452-459. https://pubmed.ncbi.nlm.nih.gov/26508622/#:~:text=In%202003%2C%20we%20published%20evidence,that%20FDR%20had%20paralytic%20poliomyelitis.
I have my masters in public health and I’m always drawn to research like this. I’m absolutely disgusted. As it turns out… None of our epidemics or pandemics are natural. Every one of them seems to be human generated. We are, in fact, our own worst enemy. I wish there were more whistleblowers out there.
GOF should be the prime suspect in all cases unless provably otherwise. Maybe that will tame the pursuits.
Strict liabilty should be attached to such. If the researchers' theory is that beating nature to the punch is "worth a mint" for the preventive therapies to ensue, then it is also "worth a mint" to Prevent GOF escape. Payments to amount to a mint. Bonds shall be posted in advance. Criminal liability for escape, signed in advance.
That might clean things up a bit.