

BREAKING PUBLICATION: mRNA “Vaccines” May Prime the Body for YEARS of Amplified Harm from Subsequent SARS-CoV-2 Infections
Landmark peer-reviewed paper reveals how mRNA vaccination and SARS-CoV-2 synergistically fuel global excess mortality and chronic illness — the “Hybrid Harms Hypothesis.”

Humanity was hit with dual biowarfare agents:
A manufactured SARS-CoV-2 virus — the product of U.S.–China collaboration, engineered through years of dangerous gain-of-function work.
mRNA gene therapy “countermeasures” — conceived under DARPA’s pandemic programs over 10 years ago.
Together, they have unleashed waves of chronic illness, sudden deaths, and unprecedented excess mortality.
Now, the McCullough Foundation’s new peer-reviewed paper — Compound Impacts of COVID-19 mRNA Vaccination and SARS-CoV-2 Infection: A Convergence of Diverse “Spikeopathies” and Other Hybrid Harms — published in Medical Research Archives — examines how these two agents interact to produce a toxic synergy we term the Hybrid Harms Hypothesis.
This comprehensive work, authored by M. Nathaniel Mead, MSc, PhD; Jessica Rose, MSc, PhD; Stephanie Seneff, MSc, PhD; Claire Rogers, MSPAS, PA-C; Breanne Craven, PA-C; Nicolas Hulscher, MPH; Kirstin Cosgrove, BM, CCRA; Paul Marik, MD; and Peter McCullough, MD, MPH, details how coronavirus infections appear to amplify the adverse effects of prior mRNA vaccination for years, creating a sustained global health crisis marked by chronic illness, sudden deaths, and persistent excess mortality.
Abstract
COVID-19 can have short- and long-term health consequences, including various cardiovascular, respiratory, hematologic, autoimmune, and neurological conditions. Although it is often claimed that COVID-19 mRNA vaccinations reduce COVID-19 severity and post-acute sequelae, these assertions are refuted by evidence of extensive mRNA immunization-related harms that appear to be amplified by SARS-CoV-2 infection, resulting in considerable overlap in reported adverse outcomes. Spike proteins from both sources persist in the human body over the long-term, leading to immune dysfunction, inflammation, autoimmunity, organ dysfunction, and overlapping toxicities. We hypothesize that the mRNA vaccinations create a persistent toxic milieu of spike protein, inflammatory lipid nanoparticles, and DNA impurities, amplifying morbidity and mortality risks commonly ascribed to SARS-CoV-2 infection. Many 2021-2024 morbidity/mortality events in highly vaccinated populations, though often attributed solely to COVID-19 illness (due to close temporal associations with laboratory-confirmed infection), were more likely to result from these interactions or “hybrid harms”. Evidence supporting our hypothesis includes studies of negative efficacy, overlapping pathologies (e.g., myocarditis and thrombosis), redundant mechanisms, and epidemiological surges in excess mortality during the Omicron era (since December 2021) in extensively vaccinated countries. Case report data indicate that spike protein production along with associated “spikeopathies” may persist for at least three years, during which a coronavirus infection could trigger a new disease syndrome that would logically be attributed to the infection based on the timing. In contrast there is a relatively mild course for Omicron infections in the unvaccinated. Ongoing spike production from prior mRNA vaccinations is likely to predispose Omicron-infected individuals to cumulative adverse effects over time. The amplified toxicities and immunopathologic effects may help account for near-synchronous waves of COVID-19 and all-cause mortality in the Omicron era. This novel framework calls for re-examining the unique immunopathological consequences of SARS-CoV-2 breakthrough infection in COVID-19 mRNA-vaccinated individuals and consideration of the implications for future public health strategies.
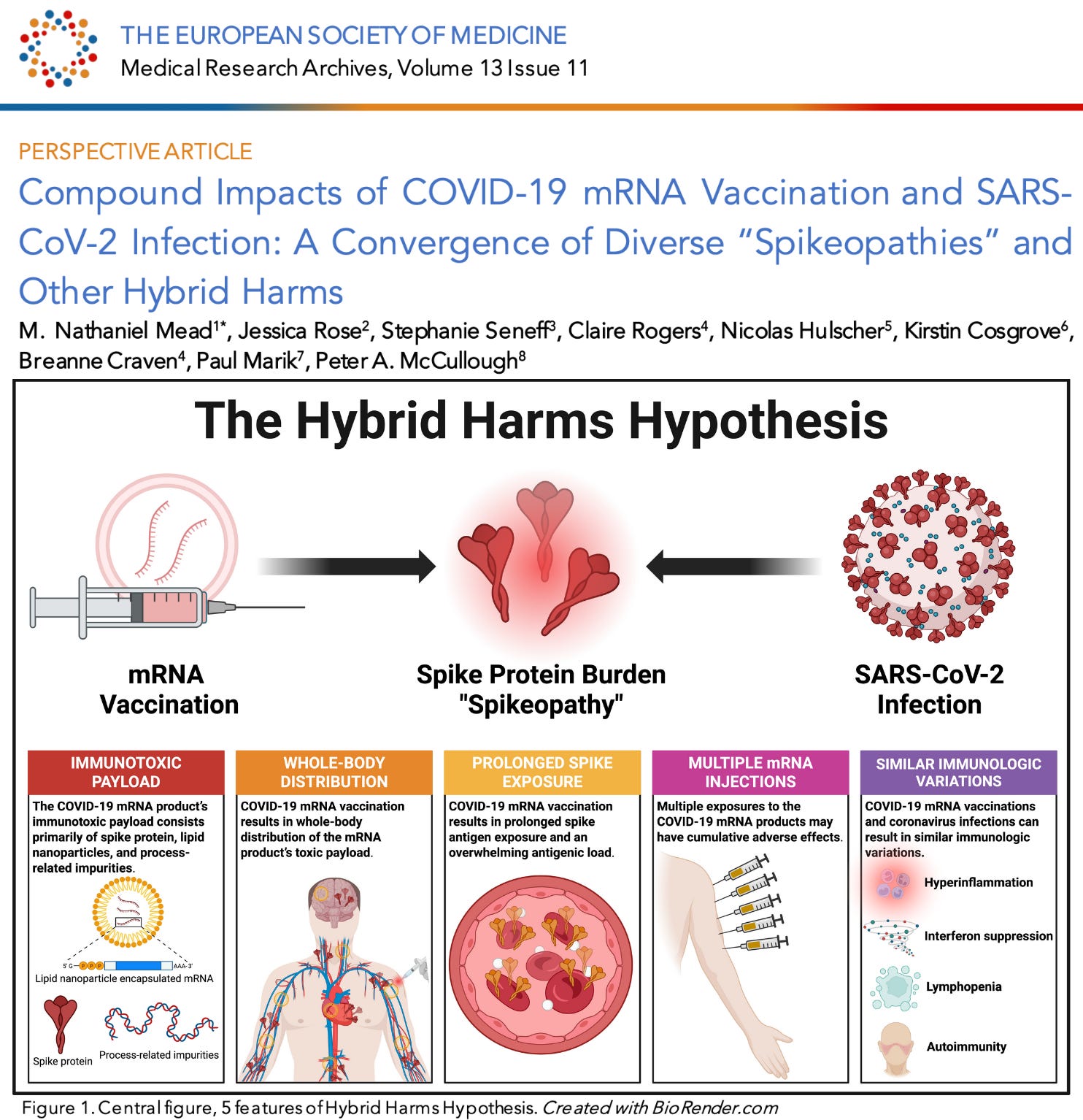
The Five Features of the Hybrid Harms Hypothesis
1. Immunotoxic Payload
mRNA vaccines deliver:
Spike protein — toxic whether from virus or vaccine.
Lipid nanoparticles — highly inflammatory and immune-disruptive.
DNA contaminants — risking genomic integration, autoimmunity, and cancer.
This persistent immunotoxic burden primes the body for greater damage upon future SARS-CoV-2 encounters.
2. Whole-Body Biodistribution
The mRNA-LNP package does not remain at the injection site. It travels throughout the body — crossing the blood–brain and placental barriers, and accumulating in heart, brain, ovaries, adrenal glands, and more. This means any infection can become a multi-organ assault.
3. Prolonged Spike Protein Exposure
Heavily modified for stability, synthetic mRNA can drive spike protein production for months — and in documented cases, for years. This persistence cannot be fully explained by prolonged mRNA stability or protein retention alone. A plausible mechanism is genomic integration of plasmid-derived foreign DNA — including the SV40 promoter and spike-encoding DNA — into human cells.
The spike protein itself is resistant to breakdown and can remain embedded in tissues long after injection. This creates a 2–3 year “Window of Vulnerability” in which each subsequent SARS-CoV-2 reinfection may amplify damage, layering new injury on top of existing spike-induced pathology — a process central to the Hybrid Harms Hypothesis.
4. Cumulative Exposure
Multiple mRNA doses stack the risk. Each shot adds to the total spike burden and deepens immune dysregulation. Infections after repeated vaccination are met with altered immune programming — including IgG4 class-switching and T-cell exhaustion — impairing viral clearance and cancer surveillance.
5. Overlapping Pathophysiology
Both mRNA vaccination and SARS-CoV-2 infection can cause:
Hyperinflammation
Autoimmunity
Lymphopenia
Interferon suppression
When these mechanisms overlap, they can be additive or synergistic — making post-vaccination infections far more dangerous than either exposure alone.
Negative Efficacy Fuels COVID-19


Multiple heavily vaccinated nations experienced pronounced surges in COVID-19 cases and excess mortality during the Omicron era, despite the variant’s substantially lower intrinsic severity. The published data show that mRNA vaccine effectiveness is negative, with several large studies demonstrating that infection risk increases with each additional dose. Evidence from the Cleveland Clinic, Japan, Israel, Qatar, the UK, Iceland, and U.S. cohorts all confirm dose-dependent elevations in infection rates among mRNA vaccine recipients. Collectively, these observations indicate that mass mRNA vaccination played a major role in driving post-rollout COVID-19 waves.
Post-Vaccine Syndromes Often Masquerade as “Long COVID”
Our paper makes clear that many conditions currently labeled as “Long COVID” are indistinguishable from post-vaccine injury syndromes, because both natural infection and mRNA vaccination expose the body to the same pathogenic spike protein, which can persist months to years after injection.
Persistent spike protein is documented in both groups, but a recent study has shown that vaccinated “Long COVID” patients exhibit dramatically higher spike antibody levels—averaging 11,356 U/mL vs. 1,632 U/mL in unvaccinated Long-COVID patients—despite no recent infection, indicating a vaccine-driven spike burden rather than post-infectious pathology.
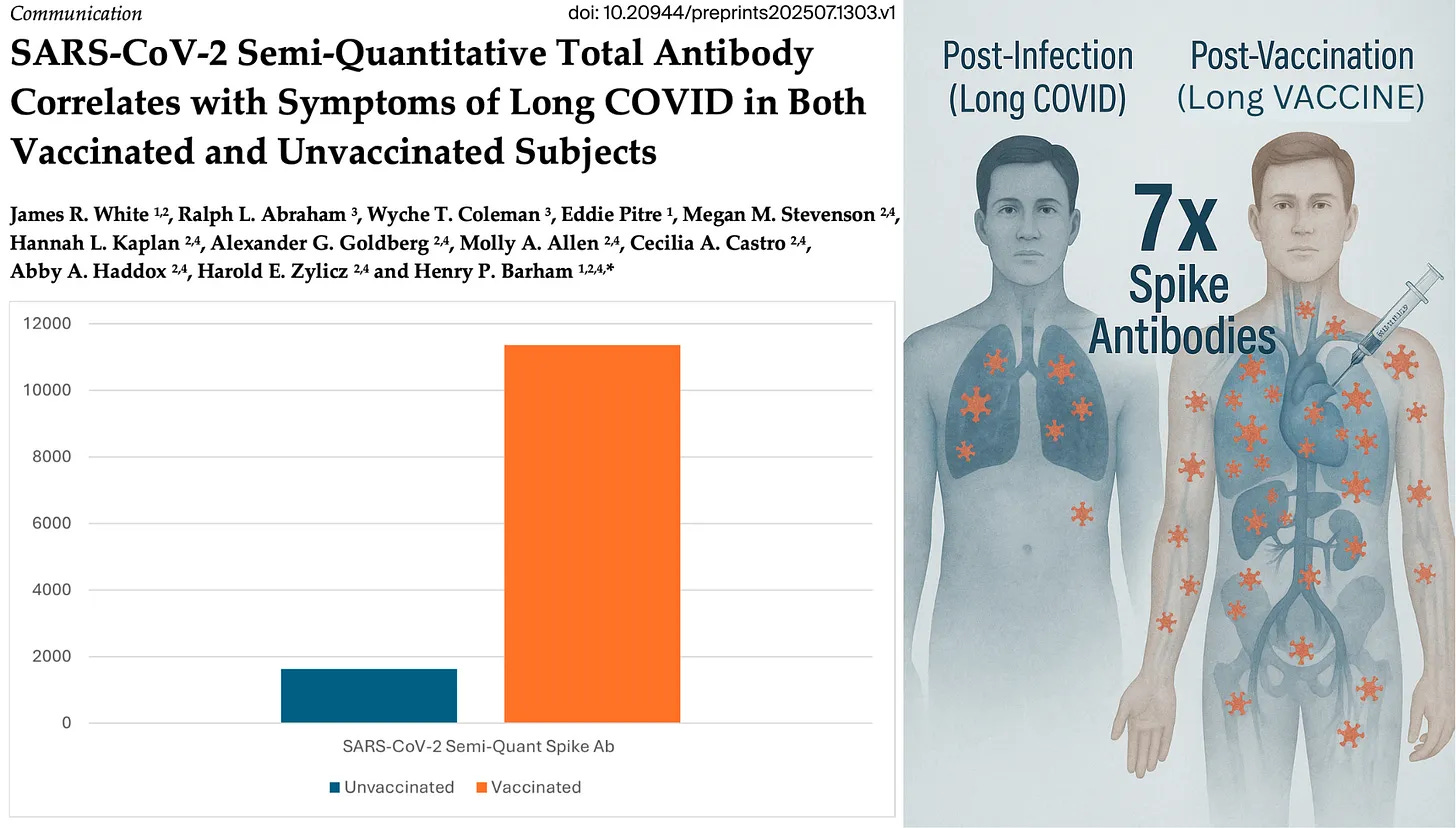

Because the clinical profiles of Long-COVID and Post-COVID-19 Vaccine Syndrome (PCVS) overlap almost perfectly across organ systems (Table 1 of the manuscript), these vaccine injuries are routinely mislabeled as “Long COVID,” thereby concealing the magnitude of mRNA-related harms and artificially inflating estimates of risk attributed to the virus.
This systematic misclassification distorts the true risk–benefit profile of mRNA products.
Excess Mortality and Misattribution
Across multiple highly vaccinated nations, sustained excess all-cause mortality continued well into the Omicron era, long after the variant’s intrinsic lethality had fallen to minimal levels. These mortality spikes consistently coincided with Omicron waves despite the variant’s markedly reduced pathogenicity.
A large proportion of these deaths were recorded as “COVID-19,” yet occurred predominantly in fully vaccinated or boosted individuals, including many whose last dose was administered months or years earlier. Reliance on RT-PCR testing further inflated COVID-labeled mortality by capturing incidental or non-causal infections, masking the contribution of underlying vaccine-related pathology.
A plausible mechanism is that prior mRNA vaccination amplified the severity of otherwise mild reinfections, due to persistent spike protein, immune dysregulation, subclinical organ injury, and the cumulative effects of repeated antigenic exposure. This interaction can convert a clinically trivial infection into a severe or fatal event in susceptible individuals.
As a result, large numbers of post-2021 deaths have been systematically misattributed to COVID-19 rather than to vaccine-infection synergy. This explains why even mild Omicron waves produced disproportionate peaks in excess mortality in highly vaccinated populations—a pattern fully consistent with the Hybrid Harms framework.
If the Hybrid Harms Hypothesis is correct, millions remain in a prolonged danger zone where each reinfection can trigger severe illness or death — a consequence of mass mRNA vaccination policy layered on top of a lab-engineered pathogen.
This has produced a sustained, global health crisis with no precedent in modern history — and still no accountability for those responsible.
Epidemiologist and Foundation Administrator, McCullough Foundation
Support our mission: mcculloughfnd.org
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.
I am very happy to be one of those with no mRNA stick pins. If I had this garbage inside me, would I worry for the next 5-10 years about what could happen? I don't know. But somebody needs to be crucified for this act or terrorism against humanity. I imagine there are thousands of somebody's on that list.
I know so many Covid vaxxed that have had Covid multiple times. That just proves your point! I had a very mild case of Covid 4 years ago and I’m unvaxed. It lasted 2 days and I got it from a triple vaxed person, only one I was around for a week prior! The entire Covid debacle is the greatest manipulation of lies and deceptions I’ve ever experienced! 🤯😳🫤